
I finally got my booster shot yesterday. I intended to get it three weeks ago, but there was so much going on continuously that I ended up waiting until I could afford to be knocked out for a day in case that happened, and because it’s always easy to give excuses for not interacting with such systems. When I finally decided to do it I got an appointment literally on my block an hour later for that and my flu shot, and I’d like to be able to report there were no ill effects beyond slightly sore arms, but I’m still kind of out of it, so I’ll be fine but if I made some mistakes this week that’s likely the reason. I also had to wait the fifteen minutes. I would have simply walked out the moment they weren’t looking, but they held my vaccine card hostage until time was up.
We now have full approval for every iteration of booster shots, including mix and match, for those sufficiently vulnerable. If you’re insufficiently vulnerable but would still rather be less vulnerable, there’s a box you’ll need to check.
I got a chance to listen to the Rogan podcast with Gupta, and have an extensive write-up on that. It was still a case of ‘I listen so you hopefully do not have to’ but it was overall a pleasant surprise, and better than most of what passes for discourse these days.
Executive Summary
- Conditions continue to improve.
- Booster sequences including mix-and-match have been approved.
- Rogan did a podcast and I listed to it so you don’t have to.
Let’s run the numbers.
The Numbers
Predictions
Prediction from last week: 481k cases (-12%) and 9,835 deaths (-11%).
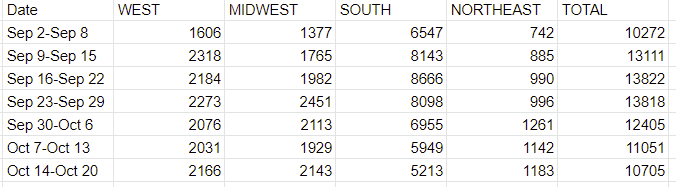
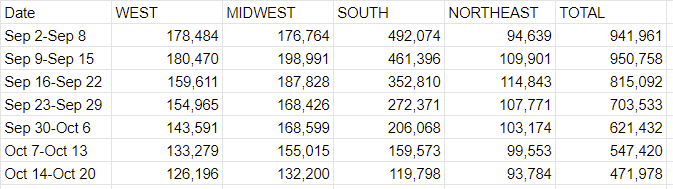
Results (from data source unadjusted): 472k cases (-15%) and 11,605 deaths (+1%).
Results (adjusted for Oklahoma which will be baseline for next week): 472k cases (-15%) and 10,705 deaths (-3%).
Prediction for next week: 410k cases (-13%) and 9,600 deaths (-10%).
Wikipedia reported over 1,100 deaths in Oklahoma this week. That’s not plausible, so I presume it was a dump of older deaths or an error of some kind, and removed 900 of them from the total.
There’s no hard and fast rule for when I look for such errors or how I do the fixes, so you can decide if what I’m doing is appropriate. Basically if an entire region gives a surprising answer I’ll look at the individual states for a large discrepancy, which is at least slightly unfair since sometimes it makes the number look ‘normal’ when it shouldn’t, but time is limited.
This is still more deaths than I expected, but given cases continue to drop I expect deaths to keep dropping. It’s possible there was another past death backlog I didn’t spot because it wasn’t big enough to be obvious.
Deaths
Chart and graph are adjusted (permanently) by -900 deaths this week in Oklahoma.
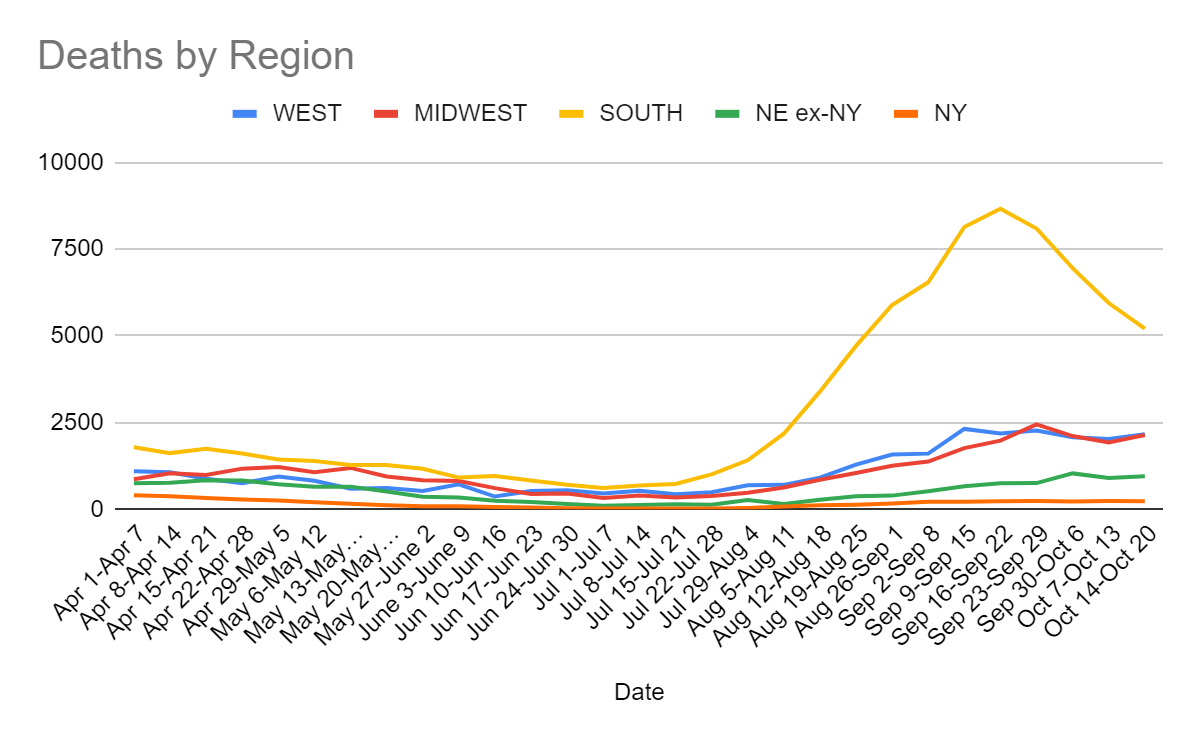
Death counts seemed higher than plausible in general even after the fix, but it’s a small mistake. Next week will tell us whether or not it is a blip.
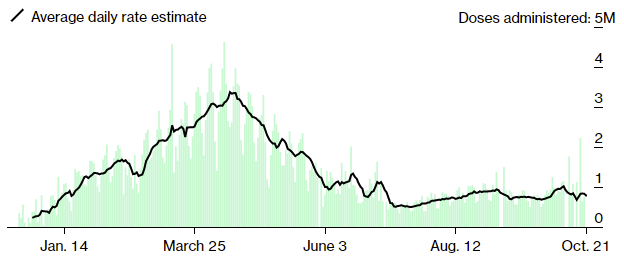
Cases
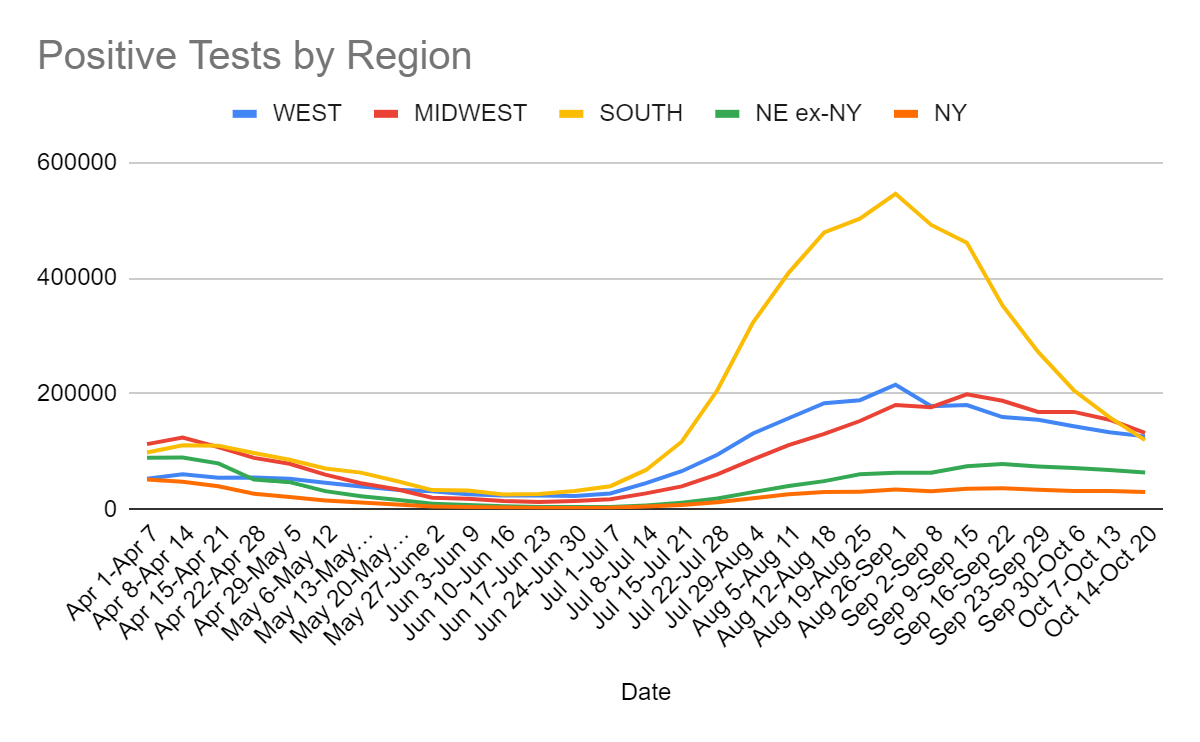
The South’s situation continues to improve rapidly, and it now has fewer cases than multiple other regions, but we see improvement everywhere. Solid improvement in the more northern states is especially promising in terms of worries about a possible winter wave. Can’t rule it out, but it seems somewhat less likely.
We are now down more than 50% in cases from the recent peak, and over the last five weeks, although regionally that is only true in the South. But we’ve clearly peaked everywhere.
Vaccinations
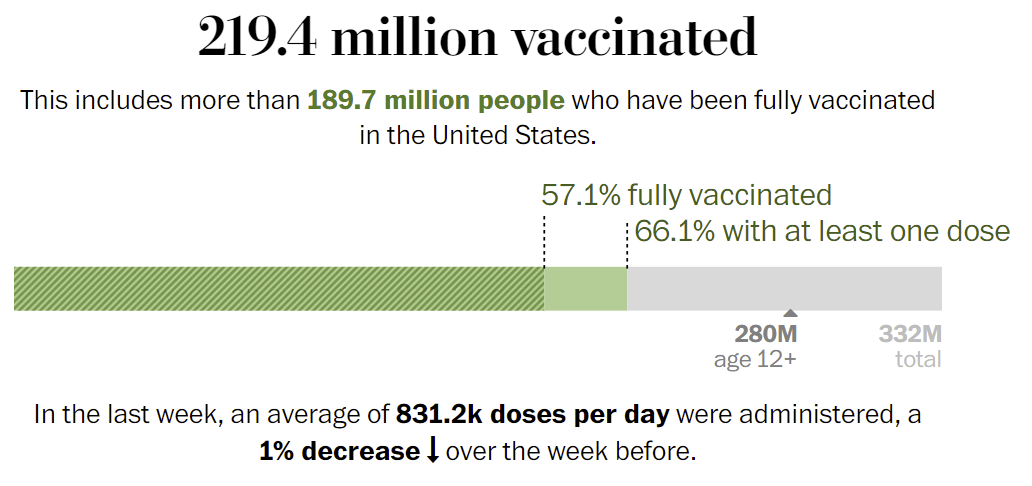
Nothing ever changes. Which at this point is good. Steady progress is more meaningful each week as more of the population is already vaccinated.
Vaccine Effectiveness and Approvals
In the words of Weekend Editor: Today the FDA formally authorized Moderna boosters, J&J boosters, and all the mix-and-match combination boosters. This is very aggressive for them!
Indeed, and congratulations to the FDA for doing the right thing, at least on this particular question. When someone does the right thing is the time to thank them, no matter how long overdue it might be.
As per procedure now the CDC gets to have all the same discussions, because if there’s one thing we need enough of it’s veto points. We’ll know the outcome on that next week.
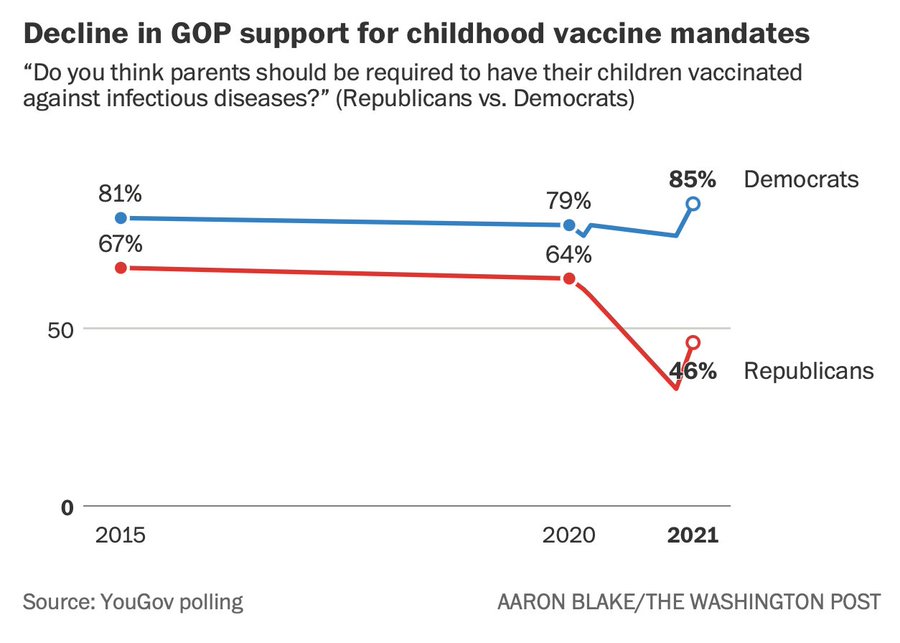
Vaccine Mandates
Support for older vaccine mandates is declining. This could end up being quite bad.
There continue to be claims that there will be massive waves of people quitting over vaccine mandates, this time in New York City. No, we are not going to lose half our cops, no matter how excited that prospect makes some people these days. We’ll find out soon enough:

On the one hand $500 is in the ‘let’s actually get it done’ range and worth it if it works, and should smooth over any general grumbling, on the other hand it’s enough that I’m pissed off that they’re getting that many extra tax dollars for what they should have done anyway.
Here’s a Zeynep thread on the psychology involved. Lot of good food for thought.
A vaccine mandate carries with it the requirement to verify that it is begin followed. This in turn means verifying people’s vaccine status and ID at various points. When does this end? Some people who based on their previous writings really should know better are seemingly fine with ‘never’ and I notice I am most definitely not okay with that for everyday activities. There will be a point these mandates \(\) everyday actions turn negative, and it’s not that far off, and then we’ll have to figure out how to unwind them. Would be increasingly happy to start now.
This post looks at vaccine persuasion in Kentucky, notes that $25 Walmart gift cards were a big draw, doesn’t seem to offer much hope that persuasion via argument would work. But have we tried bigger gift cards?
California state works are somehow vaccinated at a rate much lower than the state average. Ignoring for the moment that they don’t seem to be doing much to fix this problem, one can draw various conclusions about how the state government operates and hires based on this. And one can wonder why, if the state is willing to impose so many other restrictions, they can’t or won’t take care of business in this way. However, the article also notes that this is comparing the number who provided proof of their vaccination status as employees, versus the number who actually got vaccinated as adults. It seems that some employees may have simply decided not to provide proof, either as a f*** you to the demand for proof of vaccination, or because it seems that if you don’t vaccinate they ‘make’ you get tested a lot but that’s free and some people like the idea of getting tested frequently, so whoops.
Washington State’s football coach is out:
So is an NHL player, and even if you oppose mandates I hope most of us think that faking a vaccine card is not a permissible response.

This is a remarkably high tolerance of importantly fraudulent behavior. Very much does not seem like a sufficient response.
Not endorsed, but noting the perspective that the unvaccinated are holding us hostage, because the threat of potentially running out of health care capacity is the reason we still take major preventative measures, and if everyone got vaccinated we would go back to normal. I find the hostage situation metaphor apt because hostage situations are mostly because we choose to care about them. Every so often, someone on a show will grab a hostage, and the response will quite correctly be ‘I’m not going to reward threats to destroy value by giving you what you want’ and I wrote a contest essay back in grade school arguing this should be standard procedure. Instead, we’re more like a DC hero who thinks that if you point a weapon at any random citizen they are forced to hand over the world-destroying superweapon codes. I will leave it to you to draw the appropriate metaphor to our current situation on other fronts.
NPIs Including Mask and Testing Mandates
From New Zealand and Offsetting Behavior comes the story of Rako. Rako offered to scale up their Covid-19 tests, the government said they weren’t interested, then when it turned out the tests were good they reversed course and decided to take what tests and capacity that did exist without much paying for them, among other disasters going on there, and hope that somehow anyone will be interested in helping with such matters next time around. It doesn’t look good. Neither does the Australian decision not to securely keep the police away from the contract tracing records.
How much should you update on a Covid-19 test? We’ve got a new concrete reasonable attempt answer that, although it still uses the PCR test results as their ‘gold standard’ and thus is underestimating the practical usefulness of other testing methods.
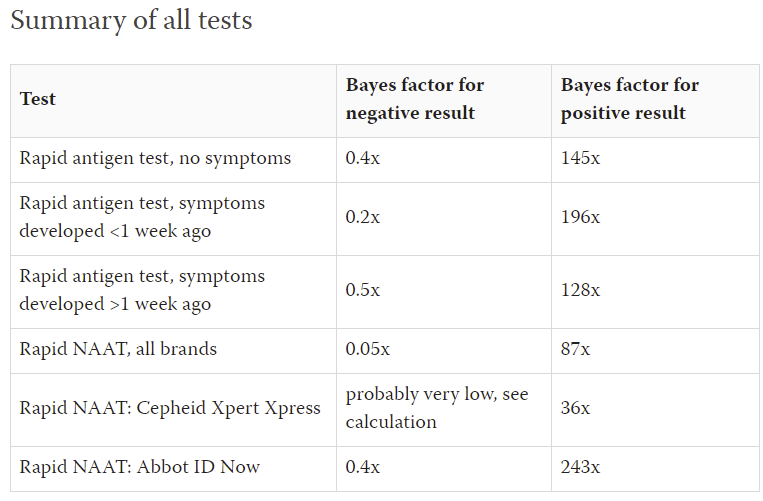
The Bayes factors for positive tests are pretty high. The ones for negative results are less exciting, but if you’re focusing on infectiousness, I believe you end up doing a lot better than this. Those who do math on this stuff a lot are encouraged to look into the details.
It turns out Rapid Antigen Testing works rather well at telling who is infectious. Here’s a thread explaining why they’re much more accurate than people thought, which is that when the PCR tests came back with what were effectively (but arguably not technically) false positives, not matching those was a failure. The fallback general official response has for a long time been something like this.
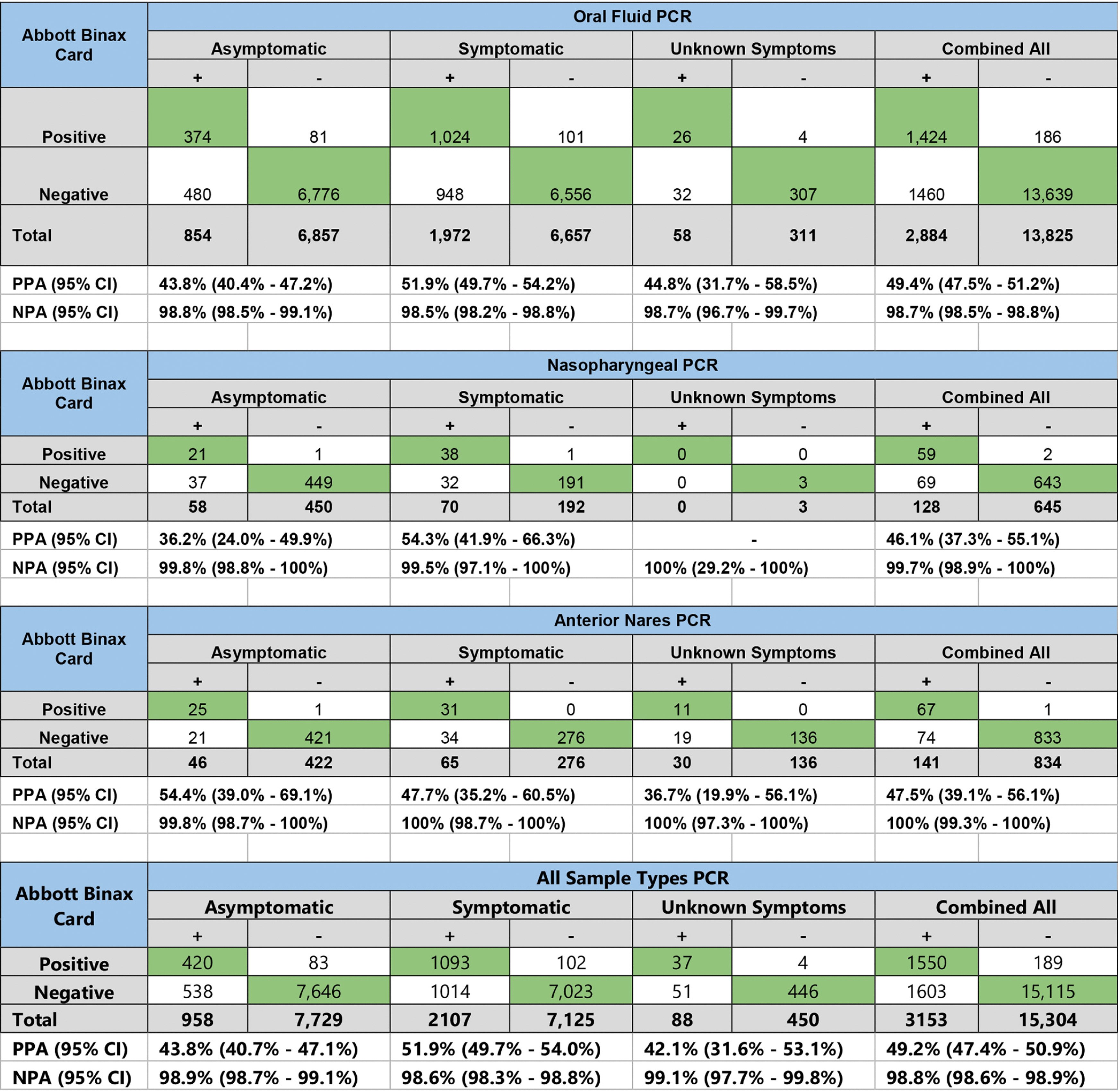
Where ‘have Covid’ is defined as ‘have or recently have had any trace of Covid’ although that’s rarely the thing that has high value of information. It is very reasonable for someone to want to know if they have (or others have) Covid, and it is also very reasonable for someone to know if they are (or others are) infectious. Different purposes, different tools, and it turns out both tools are highly useful. The mistake we made for over a year was saying that because people might also want to know if they have Covid, the test that is very good at detecting infectiousness and less good at detecting Covid was illegal, so we should instead not test at all or use a test that was more expensive, slower and less useful in context. It is good that things seem to be coming around a bit.
Restaurant that isn’t as good as Shake Shack lets people in, is now told they are out.
This was only a temporary shutdown of one store, since they only have one store in San Francisco. Depending on exactly where their stores are, this could be a very smart move, as it wins them massive points with the outgroup.
Permanent Midnight
Some of us think the ultimate goal is to become complacent about Covid-19 once it’s no longer a major threat, and return to our lives. Our official authorities say, madness.
This is an explicit call for vaccinated children to be forced to mask permanently. This is utterly insane. If not them, then who? If not now, then when?
I sincerely hope the kids neither forgive nor forget that this happened to them.
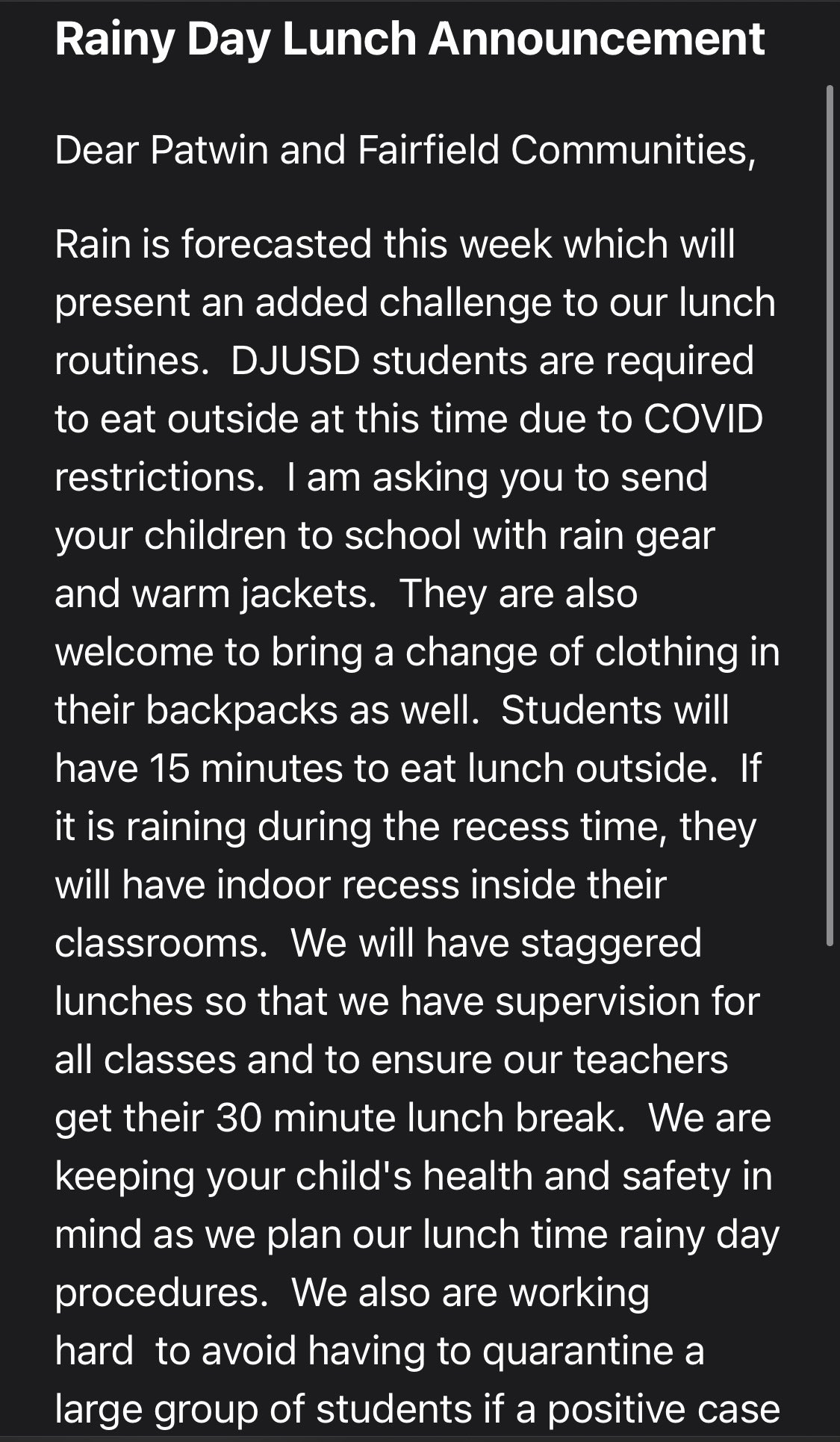
This also brings up another of my humble proposals of ‘maybe we should teach children that skipping a meal every so often is fine, so they have that valuable skill in life that’s done me worlds of good’ but mostly it’s that they are literally forcing children to go outside in the rain to eat.
Remember.
Here’s Sam Bankman-Fried going over why calls for large permanent interventions are nowhere near ever passing cost-benefit tests, and giving an attempt at a calculation and thus an opportunity to nitpick and refine.
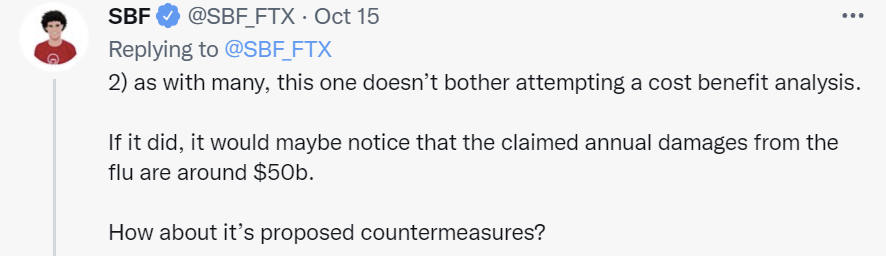
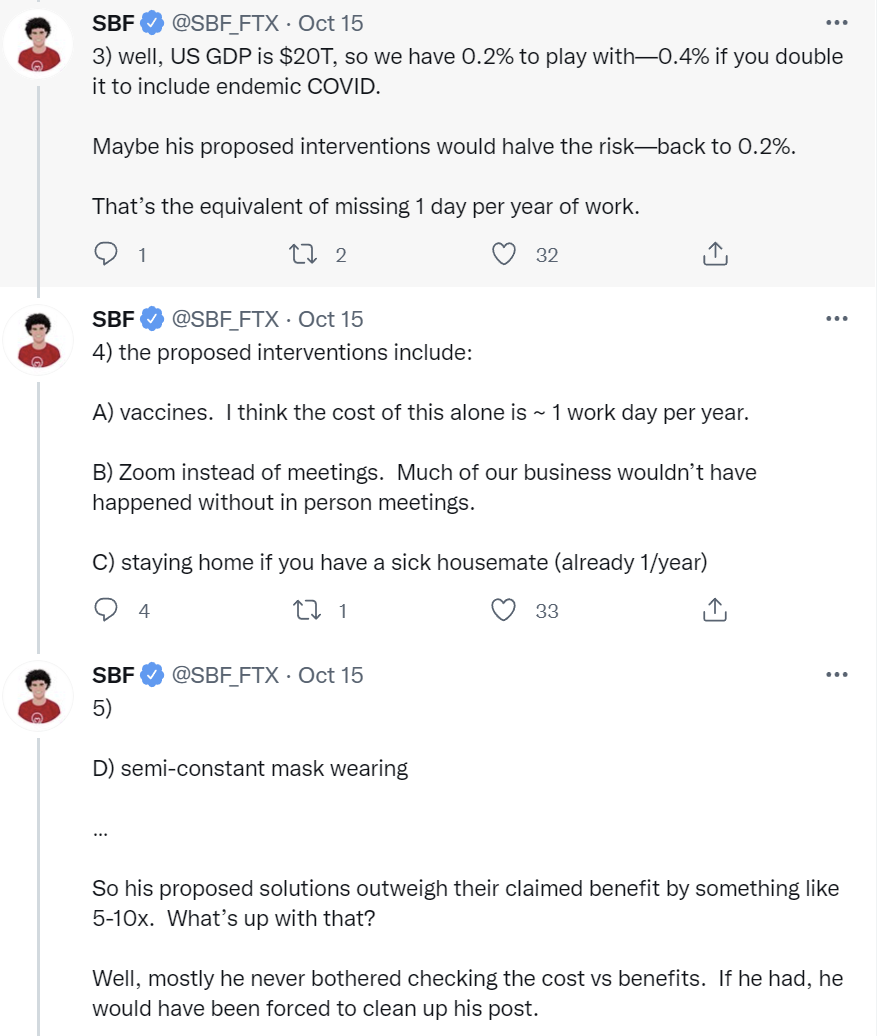
Semi-constant mask wearing costs a lot more than 0.4% of GDP. I don’t know exactly what you’d have to pay people to get them to wear masks indefinitely (with no other benefits) but I’d be stunned if it’s under 1% of consumption. Even if we knew it would work on its own with no help I have no idea why you’d even consider this.
Staying home if you have a sick housemate, to me, seems mostly like a good idea even before Covid-19. You can call this a cost of one day per year, but you have to make a bunch of assumptions to get there. Days of work can’t be fungible, so taking a random day off means your productivity is lost and can’t be made up later, and there aren’t substantial benefits from taking that extra day off on the margin. But that’s kind of weird, since if there was such a big net loss from losing a random day of work it strongly implies you’re not working enough at the baseline. And it seems likely to me that you save the office collectively a full day of productive work (since being low-level sick makes work less effective on top of less fun) by avoiding additional infections.
The exception here would be if work on that day can’t be done from home, and isn’t fungible with either other times or other people, so you lose something close to a full day’s productive value. I think that is rarely the case, and that Sam’s history of being stupidly productive at all times makes this a blind spot. For most people, my model says that either (A) you can mostly get others to cover for you without too much loss and (B) most of the work where this isn’t true can be done remotely for a day or two.
Zoom meetings are a mixed bag, but this week I had my first work in-person meeting in over a year and it was incredibly more productive than a similar Zoom meeting would have been. There are big advantages the other way, so this won’t always be the case, but I strongly agree that giving up on seeing people in person is a productivity (and living life) nightmare that costs way more than we could plausibly give up. But on the margin more Zoom meetings than 2019 is good actually.
That leaves the vaccines, which he estimates at a day of cost, and I don’t understand this number at all. Sometimes the vaccine will knock one out for a day, but this does not need to be the case and I wrote most of this the day after getting my booster shot. Over time, we’ll figure out the right dosing and regimens and the side effect impact will decline, and you can plan ahead so you choose a day when it’s not that expensive to be somewhat out of it.
If we end up passing a ‘everyone must miss a work day after the shot so everyone feels permission to get the shot’ law then it could end up costing a day, I guess, but also giving people some paid time off at the time of their choice that they plan for seems like it isn’t even obviously a bad idea?
Rogan Versus Gupta
I got the chance to listen to Joe Rogan’s podcast with Dr. Gupta. It’s a fascinating combination of things, some of which are great and some of which are frustrating and infuriating, from both of them.
The opening is a discussion of why the two of them were willing to sit down together. Gupta sat down with Rogan to try and understand Rogan’s thinking process and because Rogan can reach a huge audience that is otherwise exceedingly difficult to reach, and to convince Rogan on vaccines. Rogan sat down with Gupta because Gupta’s public changing of his mind on marijuana (which they talk then about a bit) revealed to Rogan that Gupta is willing to look at the data, change his mind and admit when he’s wrong.
In this past, both of them acquitted themselves well. The central point here was well taken. On its surface it was about the potential of marijuana and why we should not only legalize but embrace it and research what it can do for us, and I’m while I don’t have any desire to use it myself I am totally here for that.
The real point was that one needs to think for oneself, look the data with your own eyes and an open mind, be curious and come to conclusions based on where that takes you, and that doing this is how you earn many people’s respect. That Gupta was here with the ability to engage in (admittedly imperfect, but by today’s standards pretty darn good) discourse because he’d shown himself in the past to be an honest broker and truth seeker acting in good faith.
They then started getting down to it and discussing the situation in earnest. Compared to my expectations, I was impressed. Joe Rogan came in curious and seeking truth. He had many good points, including some where he’s more right than and where he was wrong, he was at least wrong, making substantive claims for reasons and open to error correction and additional data and argument. He was continuously checking to see if Gupta’s story added up and whether it lined up with Rogan’s model of the world in general, but was quite open to learning more.
Like any discourse or debate, there were many ways all participants could have done better.
Several people have noted that Joe Rogan is drawing a distinction between vaccines, where the burden of proof of safety is being put on the vaccines, and on various other things like Ivermectin, where he largely puts the burden on others to show they are not safe, and holds them to a very different standard. In general, it seems like Rogan is hunting for an angle whereby the vaccines will look risky. Not full solider mindset, but definitely some of that going on.
It’s worth noting that Rogan explicitly states in minute 59 that the risks from the vaccines are very, very small. This is despite Rogan listing off people he claims to know who had what he thinks are deadly serious adverse reactions, so it’s not clear to me that he in his position should even believe these risks are all that small.
Rogan’s point that Gupta is at far greater risk as a vaccinated healthy older adult, than a child would be unvaccinated, is completely correct and a kill shot when not tackled head on. None of our actions around children and this pandemic make any sense because we refuse to reckon with this. Gupta has no answer. The response ‘I think you have to draw a distinction between those that have immunity and those that don’t’ is not a meaningful answer here – saying the word ‘immunity’ and treating that as overwriting age-based effects is Obvious Nonsense and Gupta is smart enough to know that. As are his attempts to move back and forth between risk to self and risk to others when dealing with kids. If he wants to make the case that vaccinating kids is mostly about protecting others, that’s a very reasonable case, but you then have to say that part out loud.
Which is why Rogan keeps coming back to this until Gupta admits it. Gupta was trying to have it both ways, saying he’s unconcerned with a breakthrough infection at 51 years old, and that young children need to be concerned about getting infected, and you really can’t have this one both ways. Eventually Gupta does bite the bullet that child vaccinations are about protecting others, not protecting the child (although he doesn’t then point out the absurdity of the precautions we force them to take), and frames the question in terms of the overall pandemic.
The question of protecting others was a frustrating place, and the one where I’m most disappointed in Rogan. Rogan pointed out that vaccinated people could still spread Covid-19 (which they can) and then said he didn’t see the point of doing it to protect others, whereas he’s usually smarter than that. Gupta pointed out that the chances of that happening were far lower, although he could have made a stronger and better case.
Gupta was very strong in terms of acknowledging there was a lot we didn’t know, and that he had a lot of uncertainty, and that data was constantly coming in, and in engaging the data presented with curiosity and not flinching, if anything taking Rogan’s anecdata a little too seriously but in context that was likely wise.
The key moment where Rogan turns into the Man of One Study seems to start in minute 62. In response to Gupta referring to the study, Rogan has it brought up. The study’s surface claim is that for some group of young men, the risk of the vaccine causing myocarditis is 4.5x the chance of being hospitalized for Covid-19. Gupta had previously pointed out that the risk of myocarditis from Covid-19 is higher than that risk from the vaccine, and tries to point out that the study here is not an apples-to-apples comparison, as it’s comparing hospitalization risk to diagnosis risk. Rogan grabs onto this and won’t let go. It takes a few minutes and Gupta stumbles in places, but around the end of minute 65 Gupta gets through to Rogan that he’s claiming myocarditis risk from the disease is higher than from the vaccine. Rogan responds that this is inconsistent with the data from the study, which seems right. Then Gupta gives the details of his finding, but his finding is based on all Covid-19 patients in general, which is consistent with this particular risk being higher for young boys from the vaccine than from Covid-19, and potentially with the results of the study.
At another point, Gupta threw the Biden administration under the bus on the issue of boosters, blaming them for daring to attempt to have an opinion or make something happen without waiting for word to first come from the Proper Regulatory Authorities, and claiming this was terrible and caused two people to resign and treating their decision to resign as reasonable (Rogan was asking about the resignations repeatedly). He equated ‘data driven’ with following formal procedure and only accepting Officially Recognized Formats of Data. I wasn’t happy about this, but the alternative would be to start speaking truth about the FDA.
My model is that Rogan’s take on vaccines differing from the standard line comes mainly from Rogan placing an emphasis on overall health and the strength of a person’s immune system, and from taking these questions seriously and spotting others not taking the questions seriously.
Rogan’s entire model of health and medicine, not only his model of Covid-19, consistently gives a central role to maintaining overall good health. People should devote a lot of time and effort to staying in good health. They should eat right, exercise and stay active, maintain a healthy weight, take various supplements and so on. This is especially important for Covid-19, whose severity seems highly responsive to how healthy someone is, with large risk factors for many comorbidities, although not as large as age.
From Rogan’s perspective, one option against Covid-19 is vaccination, but another option is to get or stay healthy. As Gupta points out multiple times, this is a clear ‘why not both’ situation, except that there’s complete silence around helping people get healthy, even though it’s a free action. It’s worth getting and staying healthy anyway, why not use Covid-19 as an additional reason to get people started on good habits? And if you’re unwilling to help people get healthy, why should we listen to you about this vaccine? Which is a fair point, you mostly shouldn’t listen to these people in the sense that their claims are not in general especially strong evidence. It’s that in this case, it’s very clear for multiple distinct reasons that they are right.
Minute 88 is when they get into Ivermectin. Joe Rogan is not happy that he was described as taking ‘horse dewormer.’ As he points out, this is very much a human medicine, regardless of how some people are choosing to acquire it, and those people are not him: “Why would they lie and call it horse dewormer? I can afford people medicine, motherf***er, this is rediculous. It’s just a lie. Isn’t a lie like that dangerous? When you know that they know they’re lying?”
So then he played the clip, and the CNN statement wasn’t lying, exactly. It was technically correct, which as we all know is the best kind of correct – it said that he said he had taken several drugs including Ivermectin. Then it said that it was used to treat livestock, and that the FDA had warned against using it to treat Covid. Now all of those statements are technically correct – the FDA definitely warned about it and doesn’t want you doing that, and among other things Ivermectin is used to treat livestock, although it is also often used for humans and Rogan had a doctor’s prescription.
Now, in context, does that give a distinctly false impression to viewers? Yes. Are they doing that totally on purpose in order to cause that false impression? Absolutely. Is it lying? Well, it’s a corner case, and technically I guess I’m going with no? Gupta’s response is that they shouldn’t have done it, but he’s not willing to call it a ‘lie’ and is denying that there was glee involved. (Morgan Freeman narrator’s voice: Oh, there was glee involved.)
Rogan asks, if they’re lying about this, what do we think about what they’re saying about Russia, or any other news story? And my answer would be that this is the right question, and that it’s the same thing. They’re (at least mostly) going to strive to be technically correct or at least not technically wrong, and they’re going to frame a narrative based on what they want the viewer to think, and as a viewer you should know that and act accordingly.
Later on comes the part that should be getting more attention. In minute 125, Rogan explains that he almost got vaccinated, but didn’t, and what happened.
- The UFC got some doses and offered one to Rogan. He accepted.
- Logistical issues. Rogan had to go to a secondary location to get it, his schedule didn’t allow it, had to be somewhere else, planned to take care of it in two weeks.
- During the two week period, Johnson & Johnson got pulled.
- Also, his friend had a stroke and Rogan connected this to the vaccination, whether or not this actually happened.
- Rogan goes “holy ****” and gets concerned.
- Another of Rogan’s friends has what looks like a reaction to the vaccine, gets bedridden for 11 days. And another guy from ju-jitsu that he knows had what looked like another issue, having a heart attack and two strokes.
- A bunch of these reactions don’t get submitted to the official side effects register.
- Rogan concludes that side effects are likely to be underreported.
- Rogan goes down a rabbit hole of research, finds opinions on shape of Earth differ.
- Rogan doesn’t get vaccinated, thinking he’s healthy and he’ll be fine.
- Rogan gets Covid-19, his family presumably gets it from him (Minute 135), it isn’t fun, but he gets over it and he’s fine, and they get over it and they’re fine.
- Rogan tells these stories to millions of people, teaching the controversy, but still advocating vaccination for the vulnerable and for most adults, but is highly skeptical about vaccinating kids and thinks people should be free to choose.
- Gupta tries to get Rogan to get vaccinated despite having been infected, while admitting Rogan has strong immunity already, which goes nowhere.
- Rogan says repeatedly that he’s not a professional, that you shouldn’t take his advice, to listen to professionals, that he is just some guy with no filter. But this includes naming The Man We Don’t Talk About as an expert.
- But of course, he knows that saying ‘my advice is not to take my advice’ mostly never works.
The first thing he mentions in his story, the start of this reversal, is when they pulled Johnson & Johnson to ‘maintain credibility.’ This is a concrete example of the harm done by that action. It contributed directly to Rogan not being vaccinated. That speaks to how many other people had similar reactions, and also Rogan then shared his thoughts with millions of people, some of whom doubtless therefore did not get vaccinated.
The bulk of his points were about side effects in particular people that Rogan knew. From his perspective, the side effects looked very much like they were being severely underreported, especially since these particular side effect cases weren’t reported. How could he not think this? From his epistemic position, he’d be crazy not to think this. He has quite a lot of friends and people who would count as part of the reference class that he’d observe here, and the timing of some of what looked like side effects could easily have been a coincidence rather than causal, but still, he saw what looked like three of these serious cases in rapid succession, in people who seemed otherwise healthy. Meanwhile, similar risks are being used as a reason to pull one of the vaccines.
He responded to all this quite strong (from his position) Bayesian evidence, combined with his good health and his model that Covid-19 was unlikely to be that bad for him, did a bunch of research that under these circumstances put him in contact with a bunch of Covid-19 vaccine skeptics, and declined the vaccine.
I strongly feel he made the wrong decision, took an unnecessary risk and would have been much better off getting vaccinated. But mostly the heuristics and logic used here seem better than blindly trusting a bunch of experts. Sometimes that gets you the wrong answer, but so does trusting the experts.
Given he continues to mostly advocate for vaccination of adults, and seems to have come around to believing the generally accepted vaccine safety profile, that both speaks highly to his epistemic process used since he was exposed to a bunch of his good friends who were peddling other conclusions rather forcefully, and also makes me think I know here he did make his mistake.
My guess (and I could be wrong, he didn’t make this explicit) is that the decision ultimately came down in large part to blameworthiness in Rogan’s mind. In the frame most of us have, vaccines are safe and effective, so if you get Covid-19 without being vaccinated that’s on you, and if you have one of the exceedingly rare serious side effects (many or more likely most of which are a coincidence anyway) then that’s not on you. The incidents with his friends reversed this for him, combined with thinking that outcomes from Covid-19 are tied to health. In his mind, if Covid-19 got him, that was his fault for being unhealthy. If the vaccine got him, that would be on him for seeing these things happening to his friends, and taking it anyway. So he did what most people do most of the time, especially when he saw the decision as otherwise only a small mistake, and avoided what he thought of as blame, and did what he could feel good about doing. And of course, the decision was in many ways on brand. But the undercurrent I sense is that yeah, he knew it was objectively a mistake in pure health terms, but not a huge one, so he just did it anyway.
One thing that reinforces this is that Rogan comes back repeatedly to individual examples of people, especially young healthy people, who had problems that happened after getting vaccinated, and says that it was overwhelmingly likely that that particular person would have been fine had they gotten Covid-19. Which is true, but it was also far more overwhelmingly likely that they would not have had the problem they had if they got vaccinated. If you trade one risk for another smaller risk, sometimes the smaller risk happens to you. That’s what a risk is. But if you instinctively use forms of Asymmetric Justice, what matters is that this particular person is now worse off, even if on net people who took such actions are better off, therefore blame.
That of course is an aspect of vaccines being held to a different burden of proof. In his mind and many others, they’re unsafe until proven safe, and that includes long term data, and the prior on ‘artificial thing we made to do this’ in some sense is stronger than any of our ‘this is how this mechanically works or when we’d see the effects show up’ style arguments could hope to be. Whereas he puts his assortment of other stuff into a different bucket, with a different burden and a radically different prior. Which isn’t a crazy thing to do, from his perspective, although I don’t see it as mapping to the territory.
They finish up with a discussion about the lab leak hypothesis, and they certainly don’t make me less suspicious about what happened on that front.
That’s a giant amount written about a three hour podcast I listened to (mostly at 1.5x speed) so you didn’t have to. It was less infuriating than I expected, and contained better thinking, and is to be hailed for its overall good faith. We need to be in a place where such actions and exploration are a positive thing, even when they make mistakes and even when they end up causing people to be pushed towards worse decisions in many cases.
In Other News
Bioethicists have profoundly inverted ethics.
No, seriously, imagine speaking this sentence out loud. Say, to whoever is listening, “We don’t ask people to sacrifice themselves for the good of society.”
Then realize that bioethicists are far more insane than that, because what they’re actually saying is, “We don’t allow people to sacrifice of themselves, or take risks, for the good of society.”
Over half of respondents to this survey report being lonely, with only a small effect from identifying as autistic. We had a crisis of loneliness before and Covid-19 had to have made it much worse, and at this point I worry about such effects far more than Covid-19.
Not Covid, but a good politician never wastes a crisis, so here’s a look into the child care portion of the Build Back Better bill. I solved for the equilibrium, and I doubt anyone’s going to like it.
As the weeks continue to blend into one another, it seems like it’s getting to be time to formally write up my lessons from the pandemic. I don’t know when I’ll have the bandwidth, but I’m authorizing people to periodically ask why I haven’t finished that yet.

Several people have noted that Joe Rogan is drawing a distinction between vaccines, where the burden of proof of safety is being put on the vaccines, and on various other things like Ivermectin, where he largely puts the burden on others to show they are not safe
This largely what the fda used to do. Vaccines are given to healthy people, treatments are given to people that sick. If that sickness has a probability of death, a treatment with lower probability of death is better.
A vaccine with lower probability of death would also have to include the probability of becoming sick as well, before it makes to take it.
I don’t understand your distinction between: “If you’re insufficiently vulnerable but would still rather be less vulnerable, there’s a box you’ll need to check.” and “even if you oppose mandates I hope most of us think that faking a vaccine card is not a permissible response.”
In both cases, someone disagrees with the bureaucracy about object-level vaccination protocols, understands that the bureaucracy mostly cares about the piece of paper, and provides the bureaucracy the appropriate piece of paper to cause the object-level action they want. What’s the moral difference?
Coworker expect to be working under one risk profile but due to fraud are working under a higher risk. Check box lying for another dose has only second order externalities like diverting a dose or appointment away from someone. A big deal in situations of real rationing but we aren’t there right now.
Agreed, presuming those faking their vaccine cards had a prior (confirmed via PCR or antibody test) COVID-19 infection and thus have the requisite antibodies in their bloodstream. Don’t see anything wrong with someone choosing to lie to obtain the piece of paper showing they do indeed have COVID antibodies.
If you lie to get a booster you take all the risk yourself. If you lie about being vaccinated some of the risk you create is put onto others.
Sanjay and Joe as co-heads of all US COVID policy would have been way better than the dogs breakfast we got.
I was proud of both of them.
(Keep up the good work, Zvi)
Thank you for a very good report on the Gupta/Rogan dialog.
Dear Zvi, I’m very thankful for the content you provide each week! Two short questions:
1. I [M30] got vaccinated with Pfizer in June & July, feeling quite bad for a week after each dose. According to the Microcovid calculator, given my lifestyle, my risk of getting Covid-19 over the course of the next 6 months is between 1-5%. Should I consider a booster shot in the upcoming weeks?
2. What is your current opinion about the FL.CC.C treatment protocols? Months pass and I haven’t yet seen a single good debunking article on them and/or the meta-analyses they rely on, and said meta-analyses seem very convincing. Assume I basically can’t rely on the healthcare system in my country (except for emergency care), and if I got Covid-19, I would have to essentially arrange the early treatment on my own. I feel lost.
1) If your lifestyle that gives 1-5% is the same as the lifestyle you’d have if Covid-19 didn’t exist (e.g. 2019) then I wouldn’t do it. If you’d feel it let you make major lifestyle changes, that’s different.
2) I don’t know enough about the FL.CC.C protocol to say, unfortunately.
Thanks. Given that the vaccines are universally accessible for anyone interested in taking one, isn’t the early pharmacological treatment (as described by FL.CCC) the single most important issue in the pandemic management? If their protocols are ineffective and based on dubious analyses, then the mainstream could demonstrate it with one good article, so why is there a radio silence? If it’s effective – as it seems to be – then the mainstream is nearly worthless and guilty of millions of easily preventable deaths.
I’ve been trying to parse the Ivermectin debate for a while now, but I still find some parts unclear. There’s a lot of obviously bad misinfo about the drug. It did not work miracles in India or Africa. It’s not going to eradicate covid. But there are still plausible arguments that it could have some treatment effect in certain dosage regimes.
The FLCCC’s latest treatment guidelines are here, on page 2:
Click to access FLCCC-Alliance-I-MASKplus-Protocol-ENGLISH.pdf
As a simple rule, I’d suggest to take their advice in reverse order. Start with their footnote #1, which tells people to get vaccinated.
I still talk to lots of people that haven’t gotten the vaccine and intend to just take ivermectin if they get sick. I think the jury is still out on ivermectin. The latest study that ivermectin proponents point to claims a 50% reduction in hospitalization for a high dose regime. I’ll discuss that more later. Just suppose that’s true for a second. You still get a bigger effect on hospitalization just by being vaccinated, there’s no sense in skipping the shot.
If you do get sick, your next best bet is the last treatment the FLCCC recommends: monoclonal antibodies. One study says those reduce the risk of covid death by 60%:
https://www.thelancet.com/journals/eclinm/article/PIIS2589-5370(21)00382-5/fulltext
The FLCCC recommends monoclonal antibodies for “patients with ≥ 5 days of symptoms” but also says these are “for patients within 7 days of first symptoms”.
I’d imagine they’re actually more effective if you can get them as soon as possible, rather than evaluating your condition on day 5 and trying to find a doctor who will give them to you before day 7.
But those drugs are in short supply. If you can’t get them, your next best bet would be the second from last drug on their list: fluvoxamine. In the Together trial, 10 days of fluvoxamine therapy showed a 33% reduction in hospitalization from covid.
https://www.togethertrial.com/flv
Now that you’ve picked one covid treatment that definitely works (the vaccine, monoclonal antibodies, or fluvoxamine), I’d move on to the middle section, where they recommend vitamins and supplements. I’m not sure any of these will actually help you, but they’re harmless. You might as well take things like Vitamin C, D, Quercetin, melatonin, and zinc.
The FLCCC recommends taking aspirin. One meta-analysis says that aspirin cuts covid death risk in half. I have no idea if this is good research or just a meta-analysis of small, crappy studies.
https://www.medrxiv.org/content/10.1101/2021.07.08.21260236v1
But covid does cause blood clots and aspirin prevents clotting. So there’s a theoretical mechanism of action and it’s a harmless drug, so the risk vs. benefit equation obviously favors taking it.
If you’re in a country where bromhexine is sold over the counter, there are also some theories that drug might help with covid. It’s probably harmless, could help.
The FLCCC also recommends anti-viral mouthwash. Again, no idea if that works, I’ve never looked at the studies. But, go for it if you want, it’s unlikely to hurt.
At the beginning of the FLCCC guide, they suggest you take Ivermectin and/or Nitazoxanide. That’s the controversial part.
There’s some small RCT evidence that Nitazoxanide reduces viral load in covid patients, but it hasn’t shown to improve symptoms.
In vitro studies have shown that Nitazoxanide (normally an anti-parasitic) has anti-viral effects. I haven’t researched this one very much, but the doses required to hit therapeutic concentrations seem higher than what the FLCCC recommends. FLCCC says 500mg, twice a day. This study suggests you’d actually want 1400 mg, 2x/day. Or 900 mg, 3x/day. Or 700 mg, 4x/day:
https://bpspubs.onlinelibrary.wiley.com/doi/full/10.1111/bcp.14619
So… there’s really no RCT evidence that drug works, but there’s a theoretical mechanism of action.
Finally, ivermectin…
Many of the earlier RCT’s have been dismissed as fraudulent or flawed. The biggest valid RCT was the Together trial, which found only a very mild effect from 3 days of taking 0.4 mg/kg on an empty stomach. There was a 20% reduction in hospitalizations that might not have been statistically significant, the error range includes the chance that was a random result.
A more recent trial in Argentina used the drug for 5 days at 0.6 mg/kg, given after a meal, which increases absorption (studies disagree how much, some say it’s a large difference). They claimed a 50% reduction in hospitalization/death, on a large number of patients:
https://c19ivermectin.com/mayer.html
But the trial wasn’t randomized! Total waste, they had 3000 patients take the drug, if they’d randomized half to placebo, they would have had statistically significant proof if it works or not.
The confounders they list go in the wrong direction to dismiss the results, like the ivermectin group is fatter than the placebo group. So… maybe it’s something.
There is also a theoretical mechanism of action, based on in vitro studies. A lot of people have said that it’s obvious the drug doesn’t work, because the dosage we’re giving patients isn’t high enough. This paper sketches out the argument:
https://pubmed.ncbi.nlm.nih.gov/32378737/
But some research was just published that questions a key assumption there — the amount needed to have an effect might be 10X lower in lung cells than in the kidney cells it was first studied in:
https://www.researchsquare.com/article/rs-941811/v1
And it showed there are synergies between anti-viral drugs. That paper studied combinations like ivermectin and favipiravir. But the FLCCC’s combination of ivermectin and nitazoxanide could have stronger effects than either alone.
I think we will eventually find some combination of cheap generic antivirals that have a fair effect on covid, 50% improvement in results or whatever. It could take years to get a valid RCT proving that, at the rate we’re going. We might not even settle the Ivermectin debate this year — all of the big RCT’s (i.e. activ-6, covid-out) are testing the same dosing schedule as the Together trial and the ivermectin proponents have moved on to saying that you need to use it at a higher dose, for longer. So it’s possible that every mainstream trial will fail but the drug’s supporters will keep pushing it at a different dose.
I don’t know how you’re supposed to proceed between now and then, whether it’s better to follow the advice of the FDA/NIH (don’t take anything unless it’s approved) or the FLCCC (just throw everything that might work at the virus).
Just my opinion, as a stranger on the internet. I hope that gives you a place to start reading and sort it out.
I’m higher on Zinc and Vitamin D than this list, I think both are clearly impactful.
The bulk of the advice doesn’t seem crazy in general, but it’s also easy to get a non-crazy conclusion on all that at this point. Nitazoxanide sounds like it’s similar to Ivermectin, in that there’s a theory whereby it could help if you squint the right way at lab tests, so maybe worth a study to check it out but doesn’t seem worth doing for one’s self.
For IVM itself, I basically don’t think you get to do the ‘well, THESE studies were frauds or bad designs for reasons we know, so toss THOSE out, but here’s the one where you can’t prove anything’s wrong, what’s up with that one?’ thing. The rate of ‘this study wasn’t real or has horrible problems’ is off the charts, and I can’t disregard that, nor can I ignore the total amount of straws being grasped for. I’d need very strong evidence if it was in study form, and this isn’t it. I’m certainly not going to count a non-randomized trial.
And given that a lot of damage from Covid is in your body overreacting in various ways, and what happens when patients get into ICU-level trouble, I’d be loathe to ‘throw the kitchen sink’ at the damn thing. You definitely do NOT have nothing to lose in that spot.
Broken link:
> Rapid Antigen Testing works rather well at telling who is infectious
Links to this post itself, rather than the external link it was probably meant to
Annoying one to have break down there, but I couldn’t quickly dig it out of my links page revision history, so for now no additional link there.
Does anyone have a good theory why England and the US are going in different directions right now regarding the number of Covid cases? We seem to have tracked each other more or less (with a bit of a delay) throughout the pandemic. Looking at Our World in Data with England and US side by side makes me think we will have cases go up again sooner than most think. https://ourworldindata.org/explorers/coronavirus-data-explorer?zoomToSelection=true&time=2020-03-01..latest&facet=none&pickerSort=asc&pickerMetric=location&Metric=Confirmed+cases&Interval=7-day+rolling+average&Relative+to+Population=true&Align+outbreaks=false&country=USA~GBR
Let’s compare the U.S., excluding the less vaccinated South, with the UK. The UK’s per capita case numbers have been about 2x those of the U.S. during the Delta wave. The UK has had a 0.3% CFR in that time frame. The U.S. CFR in recent weeks has been around 1.2%. That is a very large difference in the CFR. Likely explanations for this: the UK started their one dose vax campaign earlier than the U.S. (their earliest vaxxed now have lower antibodies, exposing them to infection but not death), the UK is currently testing more per capita (catching more fish in a finer net), the U.S. vax level is lower than the UK even when excluding the South.
I’m not going to try to predict a potential new surge, since my last prediction went badly wrong–I predicted peak Delta deaths in the U.S. at 60% lower than last summer’s Covid wave. I didn’t make adequate allowance for regional heterogeneity, among other errors.
Thanks Craken. That is helpful.
So we have to explain two things. (1.) Why does England have so many more per capita cases that are (1a.) increasing? and (2.) Why does England have so many fewer per capita deaths that are (2a.) staying the same/barely increasing?
Better testing in England could explain 1 but not 1a and I think doesn’t help 2 or 2a
More vaccine waning could explain 1 and 1a and 2a but probably works against 2
So maybe the hypothesis is something like more early vaccination in England helped lower chance of death throughout but now we are seeing the effects of waning in England that does lead to infection if you test enough but doesn’t seem to do much to death. The US may not follow that path because our vaccinations and “natural” infections are more recent and our testing not as robust to catch infections without serious consequence. Our deaths remain higher because we still have a population (although it is rapidly going away) without immunity at all and those are by and large the people that are dying.
The case for upcoming increase in cases in the US like what is happening in England would be that our immunity profile is more like England than we think. We will essentially get everyone antibodies and antibodies work pretty similarly no matter what the source. That will make death rare but mild infection common. The situation in England now is everyone’s future. If you test enough you will find it a lot of places, especially as it gets colder but it is no longer very deadly.
Thanks for the reply, Zvi. Given that the vaccines are universally accessible for anyone interested in taking one, isn’t the early pharmacological treatment (as described by FL.CC C) the single most important issue in the pandemic management? If their protocols are ineffective and based on dubious analyses, then the mainstream could demonstrate it with one good article, so why aren’t there any? If the protocols are effective – as they seem to be – then the mainstream is nearly worthless and guilty of millions of easily preventable deaths.
When I Googled to try and figure out who this referred to and what they were endorsing, the only concrete thing I got was “Ivermectin.” I admit I didn’t try hard to find anything additional, but that’s why I said “I don’t know” – I don’t want to judge a protocol whose contents I don’t even know.
As for Ivermectin, I would not take it to treat Covid-19 (although I would of course take it for other things that it treats) and it’s been discussed quite a bit by mainstream sources. If you don’t find their responses on that compelling, that’s up to you, but there’s been plenty of discussion on the merits and I do not see how ‘one good article’ is somehow missing here.
I think this is the group: they published (and keep updating) protocols for treating and prophylaxis, search for MATH+ protocol (not sure I can post links here).
Meta-studies do look convincing, and some treatments they propose for hospital cases (steroids for example) are already widely used everywhere.
I heard one of them rant about “supportive care only” policies at the start of the pandemic and physicians not being able to use their experience (see massive inflammation — use steroids) to steer away from mandated protocols. It is rather ridiculous to have a strict protocol when nobody knows what to do anyway.
Steroids are now used after an RCT has shown effectiveness. The doctor claimed that that RCT run a rick on not showing the signal because the dose they used was so much smaller than what FLCC recommended only the size of the study salvaged the result. If the study failed, steroids would not be used for much longer.
I think implicit in Rogan’s view of the world is the view of future potentialities – if something _were_ to go horribly wrong with with the vaccines, what is the confidence in the government communicating the situation, be willing to do anything useful, or not make things many times worse? I can imagine a worldview of many Americans where most levels of government don’t really care for public safety (remember CHAZ, defund the police?), irrational and apolitical health policy is dominant, and a month ago, the Biden admin looked at the potential of 20 years of investment in Afghanistan, an entire country, falling back into barbarism and kinda shrugged and said “hey what ya gonna do”. I mean, from the Reuters transcript of a call between Biden and Ghani (“I need not tell you the perception around the world and in parts of Afghanistan…there is a need, whether it is true or not, there is a need to project a different picture.”) you substitute the relevant keywords for their VAE counterparts and, it could be argued, this is pretty much the type of response that could be expected from this administration. Whether this is true or not, it’s not an irrational position.
Not an American, but this was one of my early hangups too in my own country. Beyond what little I could do with respect to actual medical research, what helped was knowing that the Israelis were going all in on vaccination, and my thoughts were that nobody has a bullshit filter quite like those guys, so it would probably be OK.
Long COVID overhyped, Joe Rogan better than you thought, lab leak cover-up likely…
Just a friendly reminder there are other options if you ever get sick of playing for Team CNN.
I’m on the verge of giving up hope for him. He eventually sees each trail marker but never considers where they lead.
Can someone help me understand Figure 2 on Page 17 of Public Health England’s vaccine surveillance report? https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1019992/Vaccine_surveillance_report_-_week_38.pdf
Case rates for over-40’s are higher for vaccinated than for unvaccinated. Yes, Simpson’s paradox, but can someone run through a calculation to show how this would work?
97.8% of British adults have Covid antibodies. This means that the comparison in that chart may be roughly characterized as between the previously infected/unvaxxed and the fully vaxxed who may or may not have been infected. Ideally the numbers ought to be divided into fully Covid naive (now only 2.2% of adults), previously infected only, vaxxed only, vaxxed plus previously infected. In the chart you reference they mix these groups. I don’t know if it’s a case of Simpson’s paradox. Might be. But each of these four groups have different types of resistance to Covid.
Thanks. The 97.8% figure appears to be drawn from a convenience sample of blood donors. Do you know of any seroprevalence estimates for the general population?
I agree that extremely high seroprevalence among blood donors is nonetheless informative. I need to think about this.
Here’s another source:
https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/articles/coronaviruscovid19latestinsights/antibodies
It looks like this more representative seroprevalence survey in the UK gives the percentage of adults with antibodies as ~93% in late August. About 3% of the population has had official infections since then. There can’t be much truly dry tinder left in the UK.
> the threat of potentially running out of health care capacity is the reason we still take major preventative measures.
Is it really? I mean it’s a nice story to tell, but it very much does not seem like this is why we take major preventative measures. At least here in Europe, masks are everywhere even though ICU utilization has been roughly constant throughout the entire pandemic, and well below additional “surge” capacity available for emergencies.
The hostage metaphor here that is adept is pointing the gun at yourself and saying “do this or I hurt myself and you wouldn’t want that”. Only, it is phrased in the equivalent “if you get corona then we are forced to care for you, so we must force you to stay at home”.
If you don’t get the equivalence – both things feel the same, but it’s a bit hard to articulate it immediately: in both case, the consequences of the the threat are a choice (do this => I choose to shoot myself, get corona => I choose to care for you).
Do you see any practical way of adopting a policy where we care for vaccinated people who get sick but not unvaccinated ones?
@Dave: I have seen some places saying they’re at least going to prioritize vaccinated patients over unvaccinated, including for non-Covid disease, because unvaccinated people are at general risk and put everyone at risk. It seems unthinkable but all alternatives are unthinkable in some sense, and I can see a 2022 world where if you don’t get vaccinated you can’t get non-emergency medical treatment and you can’t get insurance. In a sense that’s the natural way to force this on people.
Wasn’t endorsing this as the situation, intent was to say that if you had this model then the argument in question was at least reasonable. I don’t think it’s the only reason, but I do think it’s a big bullet in the gun without which the whole case might fall apart – if the worst case scenario was NBD that changes things.
That happened late today.
After 7 hours of data presentations along similar lines to what the FDA saw last week, the ACIP voted to recommend boosters in the same groups for the same reasons. Late this evening, CDC Director Rochelle Walensky made it official.
There was some talk of trying to guide people toward or away from specific boosters. E.g., young women away from a second dose of J&J due to thrombosis risk, or young men away from a 3rd mRNA vax dose due to myocarditis risk. In the end they didn’t do that, possibly because most doctors (and some pharmacists) will already know that and steer accordingly without official guidance.
So: boosters all around, more or less. The guidelines probably hit about 60% of the US adult population. Even overweight (25 < BMI ≤ 30) but not obese is on the list.
The next step is pediatric EUAs for kids age 5-11.
What’s interesting is that the last line gives the impression that the reason kids aren’t approved is that the people who approve things have limited capacity to hold meetings and it’s a binding constraint right now? Is that right?
That’s partly correct. (Would it be weirdly ironic if I said “technically correct, which is the best kind of correct”? Because I really want to say that back to you. I mean, it’s a good line, after all.)
There are a couple of other correct things that have to be considered together with the meeting frequency. I make it out to be something like 6 big steps, only 1 of which is the committee meetings:
First, the submittors have to run a clinical trial. That’s minimum 6 months of follow-up to establish safety for something like this. In the case of cancer trials where you’re trying to prove marginal superiority (or at least non-inferiority) compared to standard of care, that can take maybe 5 years to see a survival difference. But let’s say 6 months here: the COVID trials are gated by the number of infections that crop up in each arm, but if there’s a fairly virulent infection rate, that can go regrettably quickly as people get infected.
Second, the submittors have to prepare what’s called a dossier: all the raw clinical data (including detailed medical reports on each individual subject), all the analyses done by the methods pre-specified in the clinical trial docs, and all the slide packages explaining what the results of those analyses mean. Those are intensively reviewed by internal scientific review boards at the submittors (they’re pretty careful and skeptical; I’ve been on those boards as well as subject to them), and by lawyers because there are always lawyers. Then you have to convince upper management, some of whom are perpetually afraid of risk, to go before the FDA or CDC. So this takes, realistically, some months. If everybody’s pulling the rope in the same direction (an unusual circumstance), maybe 2 months. But sometimes longer.
Third, the FDA and CDC first throw away your analyses and your explanations. They reanalyze the data themselves, using their own statisticians and the pre-specified software right down to version numbers, according to the clinical trial protocol. Then they compare their results with yours. If there’s a mismatch, you typically get a letter that isn’t called a WTF Letter, but probably should be: it instructs you to withdraw your application or they’ll deny it, which is a permanent black mark that you basically can’t recover from. If, on the other hand, their results match yours, then they’ll prepare their own slide decks explaining what the analyses mean. Those may or may not match your explanations.
Fourth comes the thing you identified: corralling all these very busy, very important people into a meeting. I sincerely mean that: they really are at the top of their fields, and getting onto one of these committees means you’re A Bit of a Big Deal. So the FDA VRBPAC and the CDC ACIP can only meet so many times, realistically, or they’ll lose the input of some of the best-informed people in the field.
Fifth is the committees don’t get to make the decision, they just recommend to the agency (FDA or CDC) what to do. There’s some internal process for what to do there, and I have no visibility into that. Normally the agencies follow their committee recommendations (the FDA maybe a bit more often than the CDC), but occasionally do not. The last couple examples have shown where the FDA and CDC actually broadened the booster population beyond what the committees recommended, which really surprised me. (Aduhelm is another example, as you pointed out, where there were several resignations when the FDA approved it despite what a lot of the committee members thought. Maybe that’s a sign that times are changing.)
Sixth, the FDA approval and CDC clinical guidance have to filter out into the medical community, so your local doc and your local pharmacist know what to do. Sometimes that requires a lot of effort. For COVID-19, not so much: everybody wants to know what to do, and is itching to get moving. So that’s good.
So it looks to me like the next scheduled meeting is Oct 26, on Pfizer for ages 5-11. I’d also love to see full approvals for Moderna and J&J. Pediatric work for ages 6 months – 5 years is, as far as I know, still in the clinical phase.
I agree sympathetically that this is all frustratingly complex and slow!
But as all the existentialists say: nonetheless, here we are. Fixing the system is a good idea, though staggeringly difficult; during a pandemic is probably a bad choice of timing.
Regarding PCR tests still being the golden standard, my theory is that they’re afraid of people switching to antigen tests entirely as those positive will never show up in official statistics if that happens. Right now presumably a lot of people are going for a PCR test if their antigen at-home test is positive, even though its kind of a pointless exercise as long as you have a few antigen tests left at home to wait out until you’re no longer infectious.
I think this is more intentionality than such folks are capable of at scale, although I do agree there are people who prefer to see more official cases whenever possible.
Does this work?
> Zoom meetings are a mixed bag, but this week I had my first work in-person meeting in over a year and it was incredibly more productive than a similar Zoom meeting would have been.
This probably varies a lot by profession. In my own experience (in IT/SD), the convenience of everyone being able to demonstrate things via screenshare is enormous. Wheras I can’t remember the last in-person meeting I found useful in any way.
I have the same take on online meetings. They function well for my line of work (IT). I can see where in-person meetings might be preferable for more touchy-feely jobs, though.
For (IT) in particular I agree that Zoom is often (but not always) superior. I believe it’s mostly a special case.
“except that there’s complete silence around helping people get healthy, even though it’s a free action”
Do you mean this in terms of doctors giving advice or instructions to patients? If so, I admit that it’s a bad thing that there’s complete silence around helping people get healthy, but it’s definitely not a free action.
Your wife is a psychiatrist and your family are medical-adjacent, right? I presume this means you have a lot of doctor friends. Ask them about their considerations when giving a lot of “you should get healthy” advice.
I predict that, filtered through their class’s natural reluctance to take controversial positions, they will tell you they don’t give their patients this advice very often because it can quickly destroy the doctor patient relationship. Better to have a smoker in three times a year and treat him for all his ailments, and to tell him once “you probably shouldn’t smoke”, than to tell him bluntly every time and have him stop being a patient entirely.
Not saying I agree with their strategy, but I am saying I agree with their assessment of the downsides, that it’s not a free action.
Agree that on an individual relationship level it isn’t a free action to push it on people. However from a public health perspective it’s a free action to help them (e.g. they’re actions worth doing anyway if you can convince people, for the individuals and for public health), and broadly saying “it’s time for all of us to get generally healthy to help fight Covid” seems like a relatively good message in terms of public relations for public health people, versus telling people to do the things we are insisting upon.
Nothing is purely a free action because opportunity costs and because people hate being told anything at all at this point, but this is as close to free as you’re gonna get.
Brilliant stuff overall, and I thank you for your efforts. Just to correct your narrative as I’m a decently frequent JRE listener: Joe’s entire family has already had Covid, and adding to his personal anecdotal evidence, they all breezed through it in his mind. Once he felt he was possibly sick with it (he thought because he played 2 sold out arena shows in Florida, and then compromised his health by spending a late night out drinking between them), he isolated from his family (he has a 14 million dollar house so that says there’s a LOT of distance in the living quarters).
I interpreted his statement as him isolating too late, and them getting it despite that – there was clearly a window for that to happen based on what I heard in this episode before he started isolating, and the timing seemed right from his statement. And if his family was immune, why would he isolate?
> If you’re insufficiently vulnerable but would still rather be less vulnerable, there’s a box you’ll need to check.
Do you have any advice on this? I attempted to schedule a booster through CVS (originally had Moderna) and was told I need to provide proof I’m immunocompromised.
I scheduled one at RiteAid, claimed I was at high risk (which according to NY rules was technically correct, best kind and all that) and was not asked for proof. From what I’ve heard online bookings don’t ask for proof.
I was attempting to book online with CVS. Fortunately once the FDA approved last week it changed and I was able to get my booster yesterday.
I successfully scheduled a booster through CVS this past week. When registering online, you’ll want to check the box that says you’re “vulnerable” according to CDC guidelines. You will also be asked to supply a date for your last shot; make sure this is at least 6 months in the past. I was not asked to prove either of these things in store.
When I scheduled on Thursday, CVS had not yet updated to allow mismatched or non-Pfizer boosters. As such, I also needed to check the box that said I had gotten Pfizer for my first two shots. In the store, I was asked to verbally confirm this as well.
When getting the shot in store, I was asked if I had my vaccine card (or a picture of one). Saying that I didn’t did not cause any issues; the pharmacist just suggested I keep a picture on hand in the future. Not having a card to hold hostage also meant I had no reason to wait 15 minutes afterward, which was nice.
I hope this is helpful, and I hope my experience maps well to your own CVS!
Childcare equilibrium guess: stay-at-home mom founds a childcare business, enrolls her own children, and gets federal funding for it. At least, this is the best case, because in practice the outcome could be that SAHMs get paid to take care of not their own but each other’s children.
Hi. I’m recovering from COVID right now and there’s very little information about whether / how long people are infectious even after their symptoms being gone. CDC still says 10 days after first positive test, but this looks like something arbitrary they decided early in the pandemic and never actually reassessed.
My symptoms came and went in 2-3 days (I did mAbs on day 2, and either they started working almost immediately or the moment I got them was coincidentally the symptom peak). Now I’m on day 6. I’ve felt completely fine for a couple days. How cautious do I need to be?
You’re probably not infectious but you can’t be sure. If you get a rapid test, that will provide good evidence – it will come back positive most of the time if you’re infectious, negative mostly if you’re not. A PCR that’s negative is basically clear sailing, but a positive one doesn’t tell you much right now.
Joining the “ask Zvi and his hive mind for advice” crowd…
I had two full days of flu like symptoms after my second dose of Moderna. NBD but would rather not repeat! Should I try to get a j&j booster perhaps?
J&J if you can get it is all around better after Moderna, if you can find it reasonably.
Slight disagreement here. (I say “slight”, because the important thing is that you get vaccinated/boosted, and then a distant second is which brand you choose.)
If you look at the mix-n-match booster presentation to the FDA, slide 22 (which is page 23, because the FDA put a header page at the front) shows the 3×3 matrix of initial vax by booster vax, giving the fold increase in antibody levels (higher is better).
For you as a Moderna vaccinee, the middle column is the relevant one:
– Moderna followed by Moderna: 10x increase.
– Moderna followed by J&J: 6.2x increase.
– Moderna followed by Pfizer: 11x increase.
So either Pfizer or Moderna will very likely give a better ab increase than J&J.
Other considerations:
For the young and female, one might want to avoid J&J because of the smallish thrombosis risk and the availability of an mRNA vaccine alternative. Small risk, though.
For the young and male, one might want to avoid Pfizer & Moderna because of the cardiomyopathy risk and do J&J instead. (Though personally, for some reason I haven’t examined yet, I think this is a lesser risk and I favor the mRNA vaccines. But I’m old enough that the risks don’t apply personally to me, so I may be biased there.)
If the side-effects from last time freaked you out so much you’re considering avoiding vaccination, then try J&J which might be less of a problem than Moderna (which was initially dosed pretty high).
Personally, I had a couple days of flu-like symptoms after the Pfizer primary series, and was happy about it. The Pfizer booster was quite mild for me.
Fair enough, then it’s a trade-off in general, in this specific situation I would still go J&J even if I fully bought that data as accurate. 6.2x is plenty.
Thank you both. I think I will stick with Moderna in that case.
Today the FDA VRBPAC met to consider Pfizer vaccines for children 5-11. It passed with 17 yes, 0 no, and 1 abstention (Michael Kurilla, who has abstained in COVID-19 vaccine hearings before).
Vaccine efficacy was very nice: 90.7% (95% CL: 67.7% – 98.3%).
Safety was good: the cardiomyopathy seen in young males is now thought to be associated with testosterone, so the age 5-11 male cohort squeaked through with no cardiomyopathy reported.
I wrote a summary with links to the data, and a bit of commentary.
Next steps are acceptance of this recommendation by FDA administrators (a few days, maybe), CDC’s ACIP committee meeting (7 days hence), and CDC administrators acceptance. Maybe vaccinations of ages 5-11 could start the first week of November.
Then we can think about full approval for Moderna and JnJ, pediatric for Moderna and JnJ, and the infant (age 6 months to 5 years) clinical trials.
We’re making progress. Now if only we could persuade the unvaccinated to get vaxed.
Could somebody evaluate the problems with that decision Toby Rogers outlined here:
https://tobyrogers.substack.com/p/ten-red-flags-in-the-fdas-risk-benefit
Is that a case of selective criticism, or are those valid problems?
– COVID-19 rates in children ages 5 to 11 are so low that there were ZERO cases of severe COVID-19 and ZERO cases of death from COVID in either the treatment (n= 1,518) or control group (n= 750)
– Pfizer’s clinical trial in kids was intentionally undersized to hide harms
– Pfizer only enrolled “participants 5-11 years of age without evidence of prior SARS-CoV-2 infection.”
– Did Pfizer LOSE CONTACT with 4.9% of their clinical trial participants?
– The follow up period was intentionally too short.
– The risk-benefit model created by the FDA only looks at one known harm from the Pfizer mRNA shot — myocarditis.
– Pfizer intentionally wipes out the control group as soon as they can by vaccinating all of the kids who initially got the placebo.
– The FDA model only assesses the benefits of vaccine protection in a 6-month period after completion of two doses. Furthermore it assumes constant vaccine efficacy during that time period.
If you can’t find a dozen completely idiotic statements on a quick skim, or can’t heuristically figure out that the source is going to be complete shit from literally the first sentence…
Today the CDC’s ACIP committee met, and recommended the CDC approve Pfizer’s vaccine for 5 – 11 year olds.
A few hours later, CDC Director Walensky approved that recommendation.
So that’s it: Pfizer is now on the table for 5 – 11 year olds!
Pingback: Covid 2/3/22: Loosening Bounds | Don't Worry About the Vase