
Yes we are. It can happen here.
THIS IS LITERAL ONE IN A MILLION AND MUCH LESS THAN THE BASE RATE WHAT THE ACTUAL FUCK IS WRONG WITH YOU DID YOU NOT SEE WHAT HAPPENED LAST TIME ARE YOU COMPLETE MORONS OR ARE YOU MUSTACHE-TWIRLING VILLIANS YOU CAN’T NOT BE BOTH, AS IN IF YOU’RE NOT MORONS AND I LOOK AT PHOTOGRAPHS I WILL SEE MUSTACHES AND YOU PEOPLE WILL BE TWIRLING THEM:



If any of them don’t have mustaches, we need to get them some clip-on ones, because while lots of people die at least they should get to enjoy the pleasures of twirling.
Yes I am fully aware that it is technically a particular rarer blood clotting disorder that is happening here and thus in that subclass it is above the base rate and that there’s an argument this might be ‘real’ in some sense and no I do not care even a little bit about any of that and no I am not going to treat this with the dignity and respect that it does not in any way even potentially deserve. There are scientific details and if you find them interesting by all means read about them but I am ignoring them because like the points They. Do. Not. Matter.
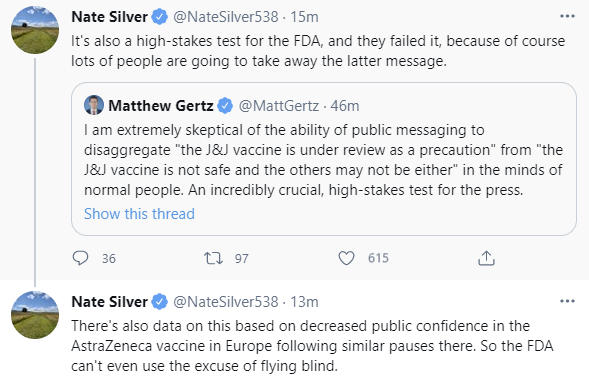
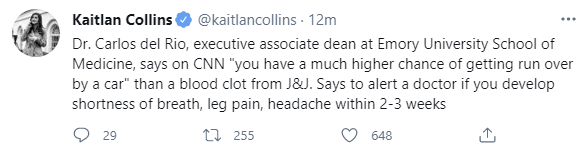
In case you were wondering how people were going to react or what this would do to public confidence, these are from less than an hour after the announcement:
I mean, they’re wrong, but I can’t fault their reasoning from where they sit, if you asked me the ‘which is more likely’ game back in 2019 I would most definitely have not have gone with ‘no really they’re doing this in a pandemic because of six cases.’
Again, seems logical to conclude they were rushed if they act in a way that would only make sense if they actually did rush.
The first time around with AstraZeneca, I could sort of understand the argument for the other side of the hesitancy effect when I squinted, that this would look like the Very Serious People Take Vaccine Safety Seriously and therefore we should now expect the people to trust the FDA more, and being untrustworthy stewards who kill a bunch of people in order to fool the public into thinking we are trustworthy is a tradeoff they thought we should make, but we ran the experiment on that hypothesis, and, yeah, no.
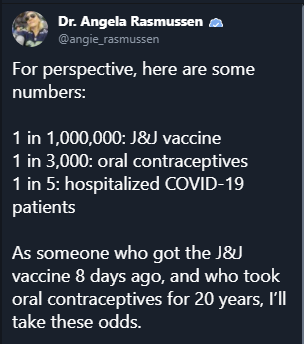
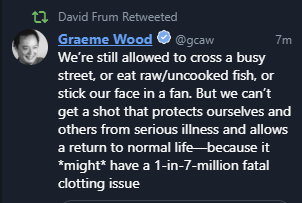
Seriously, people are not so stupid:
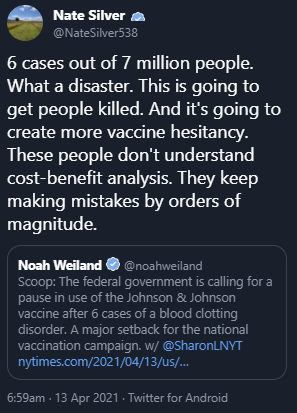
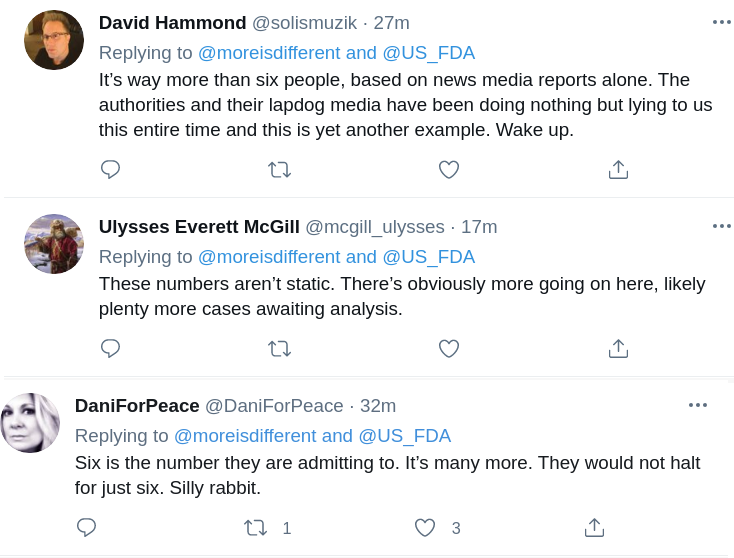
Also, when you keep saying loudly that any adverse things that happen will destroy your credibility, consider your credibility preemptively destroyed already because you’re either right or wrong:

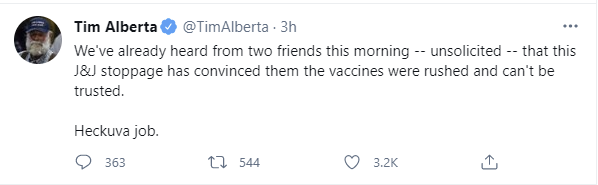
This is going to permanently supercharge the anti-vax movement, not only on Covid but also in general, and kill a huge number of people. Over six cases. Note deaths. Cases. Six.
You know how many people died?
ONE. F***ing ONE.
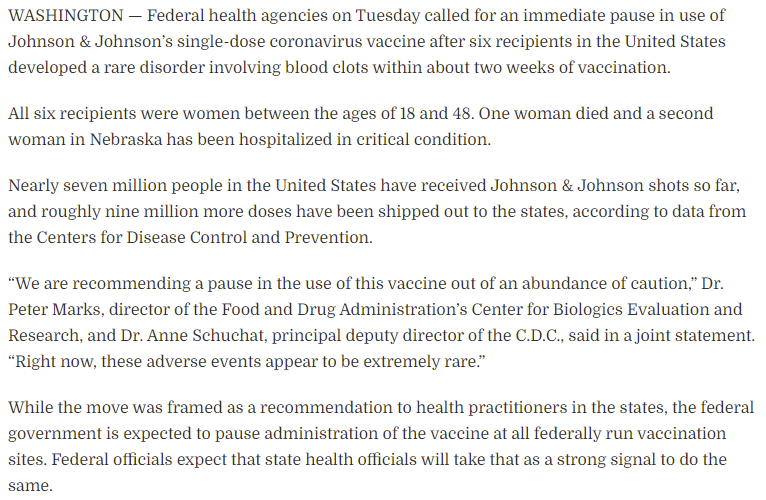
No, this was not ‘going to come out.’ It was going to completely correctly get ignored. All they had to do was put it in the list of side effects and note it was extremely rare.
This is the Washington Post’s attempt to chronicle what was going through their minds, it’s sympathetic but doesn’t make the decision look any less absurd if you actually think about the physical situation at all or how real people would react to it.
If I had to steelman the case being made, it’s a combination of believing that acting over-the-top paranoid about side effects makes people feel more confident rather than less confident, that a pause to inform people can meaningfully impact care for this rare type of blood clot, and thinking that until one looks at the data who knows how big the problem might be and one shouldn’t assume the math is right until you check it, so we should halt and catch fire for a day and then quickly convene a meeting to confirm that this is only going to kill one person in six million.
Even in a world in which the initial pause wasn’t crazy, there was a meeting the next day to go over the information, and the decision was made to wait 7-10 days and then meet again without making a choice about the pause (and obviously, here, if you choose not to decide you still have made a choice). They didn’t even make the ‘compromise’ decision of halting for young women (and yes, ‘people who are in the subpopulation that is often on birth control which causes orders of magnitude more blood clots than this seems like it’s a hint on what’s happening) and continuing for everyone else, since you can then swap doses between different groups and keep up your pace of vaccinations while you ‘investigate further’ whatever that means here. The failure to at least make that decision is obviously completely bonkers even if you somehow think the initial decision to halt and catch fire was reasonable, as laid out in this thread by someone who supported the first decision but at least supported the ‘compromise’ option at the meeting.
Here’s an argument that this isn’t so bad in the United States, as it will mostly only destroy faith in Johnson & Johnson, rather than faith in the mRNA vaccines as well, or all vaccines generally:
FDA Delenda Est. The FDA must be destroyed.

At a minimum, while we prepare to do that, we can at least implement Tyler’s modest proposal.
Let’s run the (other, not equal to one or six) numbers.
The Numbers
Predictions
Prediction from last week: Positivity rate of 5.9% (up 0.4%) and deaths decline by 8%.
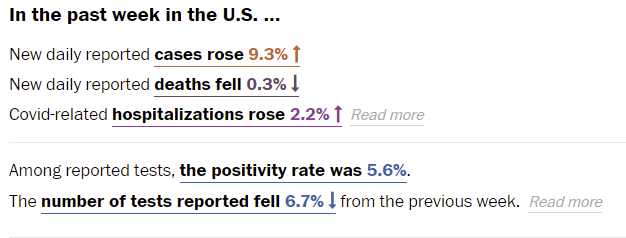
Once again Washington Post’s numbers baffle me, although this being six rather than seven days later makes them not impossible. Somehow tests fell, cases rose, and the positivity rate barely budged.
A key question whenever one gets good news on deaths is whether this is good news or whether it’s time shifted. If it’s cases shifting into the future, it means the next week looks doubly worse and on top of that you were fooled by what looked like a downward trend. Similarly, bad news can be a mirage from old cases. It now looks like the death rate decline has stalled out, which is unfortunate.
Predictions for next week: Positivity rate of 5.8% (up 0.2%) and deaths unchanged.
Deaths

| Date | WEST | MIDWEST | SOUTH | NORTHEAST | TOTAL |
| Feb 25-Mar 3 | 3834 | 1669 | 5610 | 1958 | 13071 |
| Mar 4-Mar 10 | 2595 | 1775 | 3714 | 1539 | 9623 |
| Mar 11-Mar 17 | 1492 | 1010 | 3217 | 1402 | 7121 |
| Mar 18-Mar 24 | 1823 | 957 | 2895 | 1294 | 6969 |
| Mar 25-Mar 31 | 1445 | 976 | 2564 | 1262 | 6247 |
| Apr 1-Apr 7 | 1098 | 867 | 1789 | 1160 | 4914 |
| Apr 8-Apr 14 | 1070 | 1037 | 1621 | 1145 | 4873 |
Half or more of the Midwest increase is quirky data in Missouri, but that doesn’t make any of this good news, and it’s likely deaths are going to now be stable or go slightly up, along with cases, until we get enough vaccinations to turn things around.
Cases

| Date | WEST | MIDWEST | SOUTH | NORTHEAST |
| Feb 25-Mar 3 | 66,151 | 58,295 | 151,253 | 115,426 |
| Mar 4-Mar 10 | 62,935 | 57,262 | 114,830 | 109,916 |
| Mar 11-Mar 17 | 49,696 | 59,881 | 109,141 | 115,893 |
| Mar 18-Mar 24 | 47,921 | 72,810 | 99,568 | 127,421 |
| Mar 25-Mar 31 | 49,669 | 93,690 | 102,134 | 145,933 |
| Apr 1-Apr 7 | 52,891 | 112,848 | 98,390 | 140,739 |
| Apr 8-Apr 14 | 60,693 | 124,161 | 110,995 | 137,213 |
Looking at this chart, it seems clear the Midwest’s problems are real. The finale wave is out in force there, even if it’s relatively tame in other places.
Given the increase in positive tests, and the report of a continued decline in test counts, I’m willing to believe that positive rates did go up ~0.4% in the past week, which Johns Hopkins confirms (although they have lower numbers on both ends than WaPo does), so the prediction miss was mostly about doing it based on Friday’s number or some similar quirk (or a math error on their end somewhere).
Things in many places other than the United States are quite bad. In India, they surpassed 200,000 cases per day and things are rapidly getting worse, and there are many other places that have big problems. Aside from the places that successfully did full suppression, the places doing actively well are the ones with strong vaccination campaigns. Facing the new strains while not keeping up in vaccinations is a very bad place to be right now.
Vaccinations

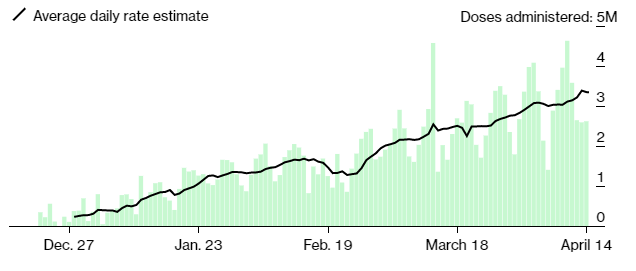
That small decline at the end might have something to do with the J&J suspension, or it could mostly be a random quirk. Either way, even without J&J, we still should be able to continue slowly expanding our vaccination rates until we hit a wall where we run out of people who want a shot put into their arm. There are signs this is starting to be an issue in some places, but mostly there’s still plenty of people eager to put the pandemic behind them.
As furious as I am at the J&J suspension, and as many people as it’s going to kill (most of which will be from disadvantaged groups and areas, which J&J’s one shot at room temperature made much easier to reach), it is important not to lose perspective. J&J was a small portion of our vaccine effort, and case growth is not that rapid, so it’s not going to kill hundreds of thousands of people, at least not in America. If we’re lucky, it will only kill thousands.
Vaccine Passport Hype
Washington Post reports on New York’s Excelsior pass, the first one of its kind. Conclusion was that it’s relatively easy to use and isn’t got reasonable privacy protections given the circumstances, but that unless you’re counting on ID to catch fraud it’s trivial to fake it via copying someone else’s pass. That sounds about right. It’s clear by now that there isn’t going to be a national system and that New York is the exception rather than the rule. That doesn’t render the questions moot, but it lowers their urgency and importance quite a lot.
Tyler’s position is that we should be planning full reopening, and that passports seem more likely to hinder that than help. That’s one of the key disagreements. Is the alternative to passports a full reopening, or is it more restrictions? My guess remains that not being able to check leads to more restrictions in the medium term (next few months), but there’s a point when that flips, and things that would have fully reopened without checking would, if given the opportunity to easily check vaccine status, continue to check that status for a while longer. We then have to balance these needs. My guess is that the ‘overtime’ period’ is 50% to last at least two months or so, but highly unlikely (<10%) to last for six, and that the ‘extra game time’ period when passports would help starts now and has at least three months to go most (75%) of the time, and there’s a decent chance (25%) it’s six months or more in at least many blue areas, so one can do a cost/benefit calculation with this plus all the other objections. Here I’m counting the extra restrictions as pure downside, because even with them the net risk is likely higher than with the pass, unless we’re checking physical cards at the door, which is a different cost/benefit tradeoff.
The other half of that is the argument from focus. If the country and discourse only have so many focus points (Imperial Focus Points!), which seems basically right, then it’s plausible that all the work on passports delays the full reopening not because of lowering the costs of not reopening fully, but by preventing the attention and blame pressure required to generate the reopenings. Doing anything at all, in this model, has high opportunity costs. I don’t think I value this as highly as Tyler but I’ve likely not been giving it its due.
Vaccines Still Work
The J&J suspension goes hand in hand with the ongoing campaign to convince the public that vaccines work, but don’t work in the sense of accomplishing anything for people. In the name of some combination of proving one’s Very Serious Person credentials, maximizing the quantity of economic harm and scaring people as much as possible, there’s a competition on how to give the impression that being out there is unsafe for the fully vaccinated.
Zeynep points us to an especially creative entry here:
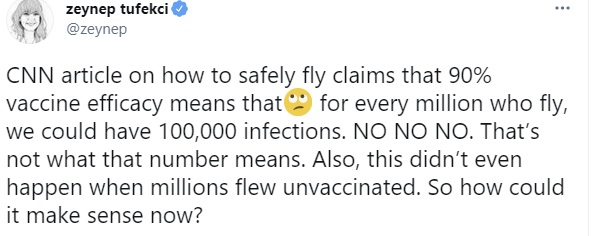
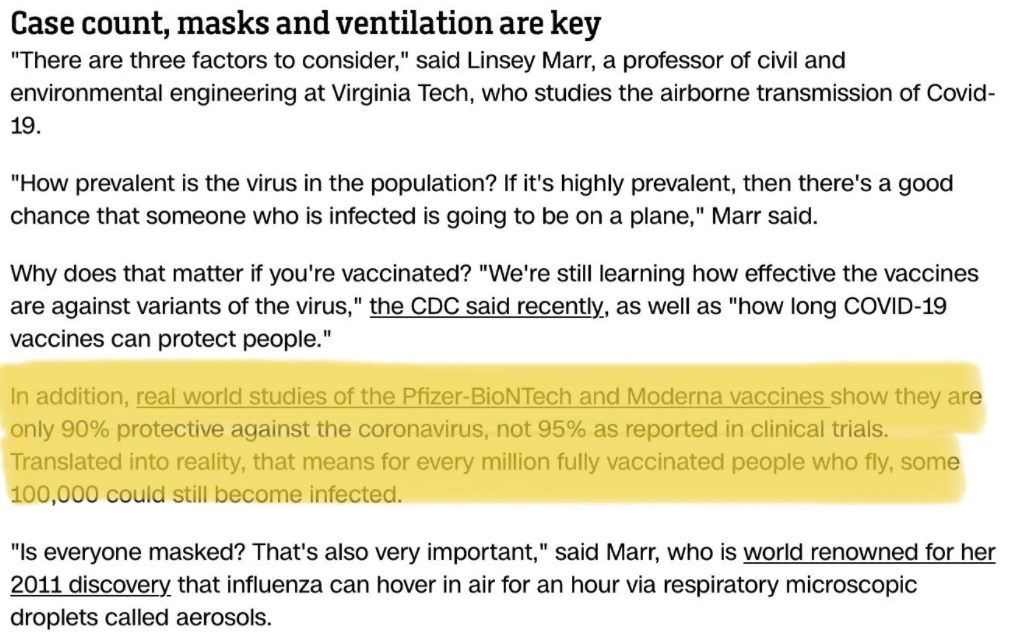
What CNN is saying might be technically correct. A model where 90% of people who are vaccinated are fully safe, while 10% remain at similar risk to before vaccination, is simplified but mostly plausible. What CNN is technically saying here is that there are 100k people who are being exposed to possibly getting infected (look around, could it be you?) and Zeynep is pointing out that this is damn well written to give the ordinary person the impression that if we didn’t Do Something About It that one in ten people who fly vaccinated would get infected, so if you’re vaccinated and fly that way there’s a 10% chance you get infected, which is of course complete nonsense.
Even without this willful mislead it’s still terrible and leads to scaremongering, but this here is something special. There should be some kind of award for such things.
Also, Nate Silver is correct here, and it would be dishonest to treat ‘we don’t know if vaccinated people can transmit’ FUD spreading as anything but gaslighting.
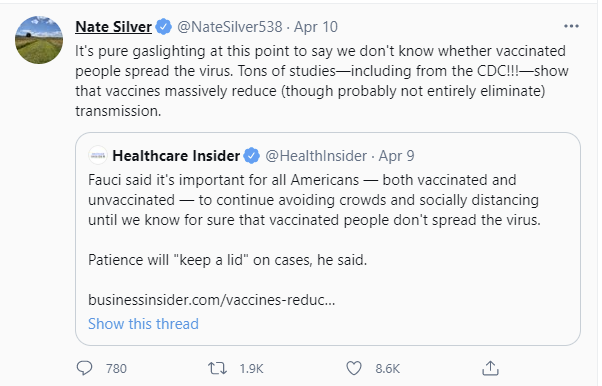
Here’s the Business Insider article linked there, which notes:
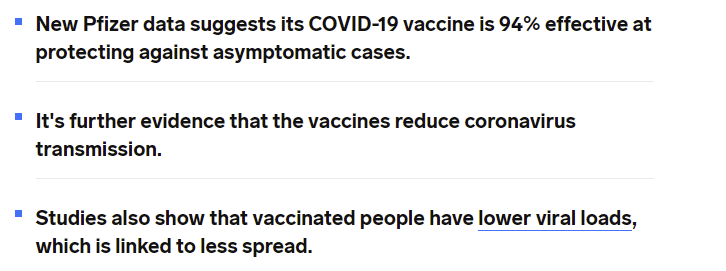
Vaccinated people are almost certainly less infectious when they do get infected, on top of not getting infected. The reduction in risk to others is ‘we don’t know’ to the extent that it might be much safer than the 90-95% range in which it reduces risk of infection.
Anyone who tells you otherwise is either lying to you, or is believing the lies told to them by others. Those who continue to treat vaccinated people as risky to others, and avoid living life on that basis, are making a choice to not live life in order to send some sort of social message or tell themselves a story about the type of person they are, or some other not-physical-reality based motivation. Or they just aren’t that into you and it’s a convenient excuse.
That doesn’t mean risk for the vaccinated is zero, precautions that are cheap are worth taking and ‘stupid stuff’ is worth avoiding, and one should follow mask norms for social reasons cause it’s really not that big a deal, but on this ‘we don’t know if it works’ thing, seriously: Stop. Just stop.
Similarly, Zeynep has a thread here about wildly misleading headlines about effectiveness of the vaccines against variants. Studies that find the vaccines work fine are being reported as ‘vaccines don’t work as well’ in a way that has nothing to do with any practical implications. The practical implications are that they work just fine, thanks, and it’s so clear I’m not even going to go into it beyond that. Attempts like this one to scare people about this are pure gaslighting.

And act more like this (video, which is living its best life):
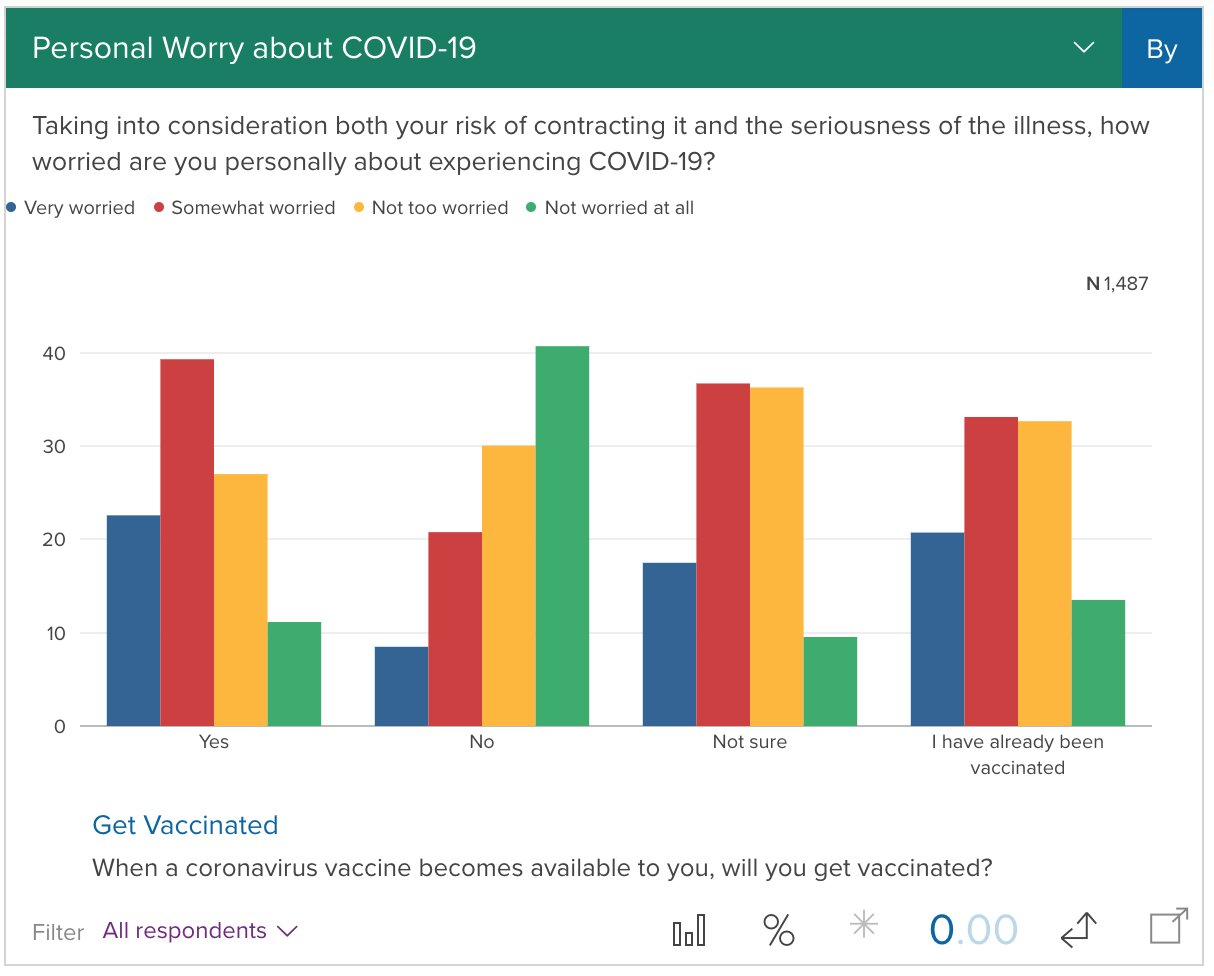
Which is why this is basically where we are:
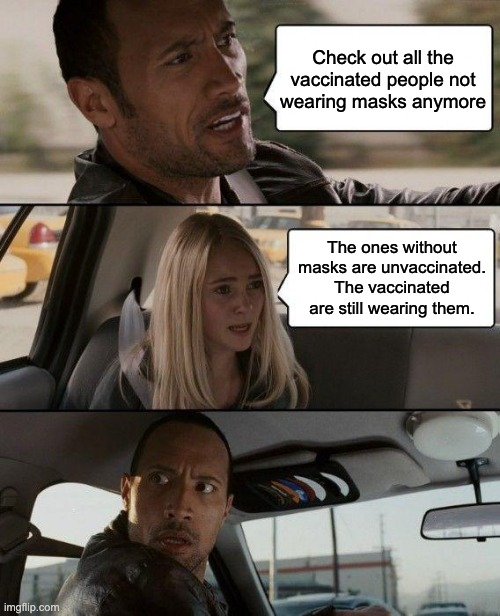
That’s before the whole Johnson & Johnson mess.
In Other News

I mean, at least it’s true.
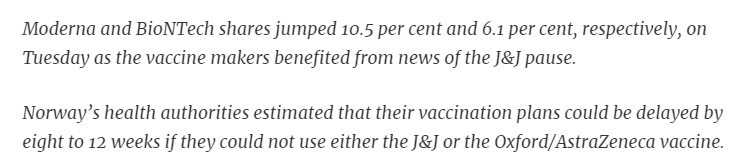
More support for first doses first. As Tyler notes, it’s too late for America to benefit from this, but the rest of the world still could. The same goes for fractional dosing. From what I’ve seen, a lot of people are having a really unpleasant day or two after the second dose of Moderna, and my strong hunch is the severity is caused by using a dose that’s twice as big as it needs to be, and it would be actively better for them to get half doses plus we’d have twice as many doses to give out.
Canadians return home via taxis from Buffalo to avoid quarantine. They did indeed solve for the equilibrium.
Australia might not open its borders even after full vaccination. The hypothesis that Australia succeeded because it was using good epistemics to make decisions is not holding up well in the endgame.
Covid Tracking Project offers thoughts on data source issues. I miss them deeply.

I think the obvious explanation for the FDA’s actions is that they are thinking “If I, knowing what I know, was hesitant to get a Covid vaccine what would convince me that they are actually safe.” Which is crazy of course but crazy in an understandable way.
I strongly disagree that they are using real means/ends reasoning, even nonsensical such reasoning, but I admit that it is possible that some people could be under similar crazy beliefs.
I wouldn’t draw a hard and fast distinction between reasoning and rationalization but I’d put this more towards the later. Still, people have stories in their heads where they’re the good guys. And persuading them often involves understanding how these stories work.
You ran a back of the envelope calculation about when herd immunity would kick in on the original strain. Any plans to rerun given B117?
If there’s 50-65% more infectiousness you need to shrink the non-immune population by 33%-50% from where it was before, since multiplication. No need to make this complicated.
[Experimenting here to see how much HTML you allow in comments.]
I wrote a piece comparing the probability per unit time risk of thrombosis for JnJ vaccinees vs other risks, such as:
dying of COVID-19 within 2 weeks,
general background rate of thrombosis in 2 weeks,
specifically CSVT thromboses within 2 weeks,
blood clots from birth control pills within 2 weeks,
thrombosis risk from AstraZeneca within 2 weeks, and
anaphylactic shock from the Pfizer or Moderna mRNA vaccines.
Conclusions:
Using the whole vaccinated population as the denominator, the risk here is lower for
the JnJ vaccine than the alternatives considered, and
Using the female age 18-49 vaccinated within the last 2 weeks population as the
denominator (pointed out by Kai Kupferschmidt), the risks are lower to comparable.
So… maybe a short pause is reasonable, if it were just long enough to do 2 things:
caution women 18-49 by either steering them to mRNA vaccines or telling them early signs
of thrombosis so they can get to an ER, and
inform clinicians NOT to give heparin to people with thromboses recently vaccinated
with JnJ (PF4-heparin antibodies and thrombocytopenia would make it worse), so use
alternative anti-clotting drugs.
It looked like that was what happened, until they decided to take 7-10 more days. Of
that, I can’t quite make sense.
Oh, and Amazon sells rather nice clip-on mustaches that can be twirled, at very reasonable prices. Just, you know, in case.
I had been looking for something like this, thanks. The subpopulation addendum made me wonder if the background risk of CSVT for women age 18-50 was any different. The Stroke article you cited also states, “Relative risk of CVT in females of reproductive age was insignificantly higher than in males”, so it looks like it would be about the same. If there are no post-J&J cases in the rest of the population, does that mean the vaccine reduces the chance of CSVT for them?!?
Or that the vaccinated population is not representative of the population in general, in CSVT risk or other risks. This is, of course, true in several ways: we’ve preferentially vaccinated the elderly and health care workers first, both of whom differ from the rest of the population. So maybe the background risk of CSVT (or CVST, in other sources) is different in the vaccinee population compared to the general population — I didn’t research that.
People were speculating, based on age & gender of the victims, that they may have been taking birth control pills and a risk synergy happened. However, I read today that all 6 victims were in fact not on birth control pills. So nothing much there.
Yes that makes much more sense. Would be nice if they found some sort of risk synergy, but seems like that might not be so easy to pin down.
So a 1/10,000 risk of death is something you should scaremonger and destroy the economy over, but 0.05/10,000 is something you should consider essentially safe and anyone who claims otherwise is gaslighting. *throws every paper on desk up into the air*
If you use Google you will see that out of the 31.4M people in the US who have gotten COVID, 564K have died. That is 1 in 57 people, not 1 in 10,000. Where does 1 in 10,000 come from?
I did notice the math here seemed quite off, but I don’t think it invalidates the point, which is that if 100% of an effect shuts down a civilization why should 5% be totally ignored? My answer would be that for various reasons it’s a lot less than 5% of the original effect, and the paper throwing is more about the attitude about the previous world.
perhaps it’s US deaths over total US population? 565k/ 330million = .00017 ~ 1/10,000 if you truncate.
Which is another way of seeing it’s a lot more than 95% reduction, as expected total infections going forward is much below infections so far.
I would guess that the rates of brain aneurysms from people’s reactions to the decision exceeds the rate of blood clots.
But seriously, the net human suffering of the reaction to the cutting of J&J, without the obvious people are going to die without a vaccine, almost certainly exceeds the net human suffering the blood clots caused. It’s insanity.
“One should follow mask norms for social reasons cause it’s really not that big a deal…”
I’m not convinced by this one. The cost of wearing masks is low IF we’re talking about a 15-minute trip to the grocery store. But if the activity I’m doing lasts hours, or involves physical exertion, or involves socializing, the cost of a mask is not negligible.
There’s also a big benefit in people visibly NOT masking, because it sends the signal that people who are vaccinated can and should behave differently! Personally, now that I’m vaccinated, I’m not wearing a mask in any place where it’s not required (and I bought a less-effective purely-for-social-signaling-type mask for those situations where it’s still required).
Yeah, if it’s not required/requested then that’s different, and you can use common sense, but I’ll do it whenever someone asks.
(Tweet author here) To be clear, no one in that video is living their best life (Heather’s doing pretty okay). They are repeating patterns that have brought and will continue to bring themselves and others terrible pain. I mostly agree with Zvi on returning to normal post-vaccine but what that tweet represents is my self-aware delusional overconfidence and relief in the 4 hours between getting the shot and really severe side effects kicking in.
To be clear as well, I meant by that note that the song was living its best life, so you should listen to it if and only if you would be interested in the best version of it.
TACTICAL NUKE INCOMING
https://www.marketwatch.com/story/blood-clots-as-prevalent-with-pfizer-and-moderna-vaccine-as-with-astrazenecas-report-2021-04-15
Seriously. SERIOUSLY. It looks like there’s a chance that ALL vaccinations will be put on pause for blood clot concerns.
We’re about to lose this fight.
Even after everything, my system-1 model still says they wouldn’t ACTUALLY pause THOSE vaccines for this, no one would stand for it, they paused J&J because we have those others, and faced with the logical consequences on this one they wouldn’t dare.
Also note that they didn’t actually BAN the vaccine, they recommended a pause, and if they tried that with Moderna/Pfizer I expect a lot of ignoring of that suggestion.
If I’m wrong, and they do pause Moderna/Pfizer over this and it actually stops being administered… well, if you haven’t gotten your shots yet there are appointments available tomorrow in many places including LA and NYC I’d really, really get on that ASAP.
Luckily, I’ve already gotten one dose of Pfizer. I’m less worried about that than I would otherwise be, but I’m still kicking myself a bit for waiting so long.
I think it boils down to what one thinks the FDA is doing. If it’s “we want to look like we care about safety, so we’ll respond to these clots and then just resume anyway”, then I think we’re fine. But if it’s “we absolutely can’t cause harm no matter what”, then they may suspend it.
The paper making this comparison is now up on a preprint server, and there’s a press release from Oxford about it.
I read the paper, press release, some criticisms, and wrote a summary. Two conclusions, shared both by the authors themselves as well as pushback from Pfizer and the NIH:
(1) The main result is that COVID-19 has a much, much higher risk of thromboses than vaccination; this is clear, well-supported, and undisputed.
(2) The comparison of mRNA vaccines vs the AstraZeneca/Oxford vaccine is unlikely to be real, for about 5 reasons the authors themselves enumerate in their conclusion. (Demographically unmatched populations, diagnosis accuracy, complications coding in electronic medical records systems in US & Europe, possibly different mechanisms of inducing thromboses, and so on.)
Whether the public and the media will be able to accept both conclusions is the issue. The risk is that they, like the reporter from MarketWatch, will just look at the numbers and decide all the vaccines are equally dodgy, thereby feeding the vaccine skepticism trolls.
You tend to adopt a charitable world view (bad decisions are caused by incompetence). The cynical worldview (bad decisions are caused by malevolence) is actually comforting here.
Assume no one is actually dumb enough to ban J&J or even Astro Zeneca because of such minor and rare effects. In that case, they are being likely banned due to influence from competitors, like Pfizer and the clots are a pretext. Pfizer is obviously not incentivised to ban itself. So we don’t we need to worry about a Pfizer ban incoming.
That’s very worrying but it’s not clear to me how representative a sample of the population those 500,000 people they got were. The collision of “has medical record” and “had an mRNA vaccine” I’d expect to be higher than that. So depending on how those tens of millions of people got whittled down to hundreds of thousands there’s the possibility for a pretty severe selection effect.
This is actually an explicit test of my hypothesis that they’ll simply bury the information and not say anything, in the sense that I said if they’d not mentioned the J&J thing no one else would have cared.
Thus, I’m going to consider this an infohazard situation to mention more broadly; not going to censor the thread but won’t be mentioning the issue more broadly in the hopes that if we don’t look at it, it will go away.
I’m flattered; never had any thought of mine called an infohazard.
I think I’m coming around to your point of view, though; from what you and Weekend Warrior wrote, I now doubt the FDA would be quite this stupid.
If uncontrolled Covid spread is still an issue in the medium to long term and annual booster shots are needed* what do you think that means for the extension of mask mandates and vaccine passports?
https://www.chicagotribune.com/coronavirus/vaccine/ny-covid-vaccine-pfizer-third-shot-20210415-sqpksyfl2fbqppfg46fxpipuay-story.html
Needed is a strong word, but we should have no issues providing booster shots if we want them. There are those who would use this as an excuse, but I can’t see this being treated that differently from the flu long term.
On the plus side, trials of boosters for mRNA vaccines vs variant viruses are already underway, and the FDA has agreed to even more accelerated approval if it comes to that. They already have an accelerated approval process for variant vaccines, like the annual flu shots for the flu virus du jour.
Of course, the optimal situation would be that we vaccinate the whole world faster, so the variants can’t become an issue. I wish I could be more hopeful about that.
One element here that makes it actually not totally obvious to assess the *purely short-term* net consequences of this pause is that the J&J vaccine is significantly less effective than the Moderna/Pfizer vaccines (the fact that J&J > 0 doesn’t settle it, as far as I can see).
I’m assuming that it’s not the case that total vaccine supply of each kind in the US is fixed — as far as I can tell, it’s instead been sort of a continuous production/distribution thing. Under this regime, with say a week of pause, roughly what happens is that the marginal people who would have taken J&J this week instead take an even split of Moderna/Pfizer/J&J but on average a week later (I guess you would expect the overall vaccination to finish 1/3 week later).
Let overall population immunity be the sum of the 0-to-1 immunities of individuals (for herd immunity, you want it to be 0.7*population or whatever).
Clearly we slow down the overall gain in population immunity by replacing +0.7 immunity by +0 immunity, and this is bad.
However, it seems that it could increase the “ceiling” population immunity % we could reach: having a vaccination-willing person get P/M means they contribute 0.9 to population immunity vs 0.7 if they get J&J.
To make things even more convenient to this argument, what if the average delay is actually less than a week? What if the prospective J&Jers get P/M doses that wouldn’t have otherwise been given this week? [i suppose to check this I guess we can look at the vaccinations per day graph and see exactly how much it dips.]
I’m having trouble seeing what back-of-the-envelope calculation to do here. Maybe the calculation would show that this is a 100 vs 1 thing, and is stupid, but this not immediately clear to me.
Also, on a personal level, I would (and would urge vulnerable ppl to) lay low, avoid covid & wait a bit if they can guarantee getting P/M over J&J. Not sure if this is that relevant though.
[I do not disagree that the overall reasoning by the govt is insane, and I do not disagree that the govt is obviously acting insanely regardless.]
The Null Hypothesis greatly appreciates this multi-bet, multi-steel man post. The Zvi is now the leading scorer in 2 of the 3 categories half way through season 1. I just wish the content of this post didn’t make my head explode. The rot within every institution that has been closely examined over the last 5 years is incredibly depressing.
Would love to get the Zvi on the scoreboard for memes as well, but don’t have a deep history reading this blog. Are there any memes coined here that i could find in regular circulation elsewhere?
We’d all much rather have functional institutions than extra FIT points, that’s for sure. Recognizing the rot, and the extent to which institutions in general or our overall culture have their own issues, is the first step in perhaps improving them.
As for memes, you can check the archive for things that potentially count, but I haven’t noticed anything. Part of the issue is that it’s only a month season, and of the people most likely to use them that would count, only Scott is producing that much content, and you need 3 uses.
Some things to potentially look for: Immoral/Moral Mazes, Simulacra Levels (both of which are existing concepts but might count), More Dakka, Out to Get You, Slack (this is likely your best shot), Sacrifice to the Gods, FDA Delenda Est (I’m presumably not the first, but again maybe?), Motive Ambiguity, Asymmetric Justice, The Symbolic Representation of the Thing, Zeroing Out are what comes to mind when I browse my post history. Again, my guess is you come up empty, but you never know.
this is very helpful. thank you. Update on FITs – season 1 will only last 1 month. new season starting 5/1. we’ve learned a lot in this beta, and some interesting rules changes coming:
1) better categories (memes will be replaced by something closer to kicking off an interesting discussion – this should dramatically reduce the value of DJT and be in more in the spirit of encouraging constructive discourse.) you will continue to be a top 5 pick in my mind as your style fits several more of the categories well. kling will post more details if he hasn’t already.
2) smaller teams – following 15 is a piece of work, so 5 or 7 is probably where this will land.
3) more teams – we’ll see if kling can get more folks interested. if so, could drive some of the desired result here of elevating the status of good faith, serious public intellectuals.
Also – thank you for the work you put into this site. I will be a regular reader going forward even if I don’t have the honor of receiving your FITs points.
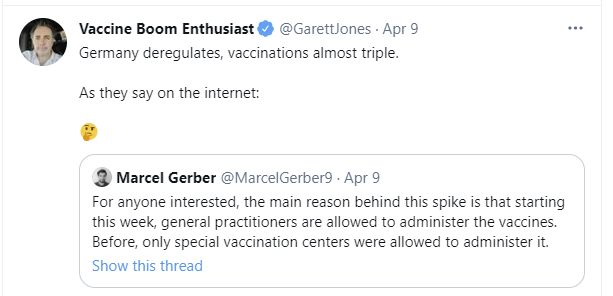
Re: Germany “deregulation” — surely this is mixing up cause & effect? Surely Germany opened up the administration of the vaccine to account for increased supply. I can’t imagine that the limiting factor in their vaccination effort was administration rather than supply, given that supply has been the limiting factor everywhere else.
And yet, with how inexplicably terrible the decision making has been overall, I’m not sure.
The Spahn problem will not be solved until the Spahn is removed from office. He was evil and incompetent long before Covid, he is evil and incompetent during Covid and he will be evil and incompetent long after Covid. The correct correction must happen by German voters in September.
Regarding cerebral venous sinus thrombosis (CVST) as the subclass of blood clots that lead to the pause in administering the J&J vaccine, you said that “in that subclass it is above the base rate “. Is it though? John Hopkins* says CVST occurs a rate of 5 in 1 000 000 be general population. Given the 6 CVST cases in 7 000 000 J&J vaccine administrations, it looks like, worst case, there would be no statistical difference with the base rate. Or am I missing something?
* “Cerebral Venous Sinus Thrombosis (CVST) | Johns Hopkins Medicine” https://www.hopkinsmedicine.org/health/conditions-and-diseases/cerebral-venous-sinus-thrombosis?amp=true
The difference is that the events seen after administration of the adenovirus vaccines is CVST *with* thrombocytopenia (low platelet count). This combination is vanishingly rare, and administration of one of the most common drugs (heparin) for treating normal thrombosis is causing patients with this particular set of symptoms to deteriorate or die.
My best guess on why administration of the J&J vaccine has been paused is 1) to wait and see if additional cases of this arise either due to delayed reporting or increased vigilance, 2) to inform medical professionals about the special testing and treatment required to care properly for those with these symptoms, and 3) to be open and honest with the public about the risks – as was done for anaphylaxis very early in mRNA vaccine administration.
Ok I was thinking the pause was a horribly impactful case of base rate neglect, and I was as upset as Zvi in the opening paragraph of this post. It’s a bit of consultation to know there is a bit more to it, even though it doesn’t justify pausing the vaccine administration.
Have you come across any source on the rate of CVST with thrombocytopenia in the non vaccinated pop? Or on the number of people in the J&J vaccinated group with CVST *without* thrombocytopenia? The CDC PowerPoint doesn’t mention either, but it seems like they are both important numbers in terms of understanding the full picture.
Not the best source, but the UK’s vaccine side effect reporting for Pfizer/BioNTech has seen 2 cases of blood clots with thrombocytopenia out of 11 million first doses and 3.5 million second doses.
That Johns Hopkins base rate is per year, while the J&J cases are within 2-3 weeks of vaccination. Also it’s important to note that CVST with thrombocytopenia is particularly nasty – currently has a death rate of 1 in 7 for J&J and around 1 in 4 for AZ – whereas only around 1 in 20 people with normal CVSTs die (and many of those who die have other serious conditions). Hopefully that’ll improve a bit now people know how to treat it.
That being said, even taking this into account it looks like the yearly risk of death from blood clots caused by birth control pills is comparable (~1-10 per million), though clots on the pill are less likely than clots during pregnancy.
That’s a good point. We’ll get a better idea of the yearly base rate of CVST with thrombocytopenia within a month (I read that most cases will happen with 40 days), but could maybe fit a curve based on the current data to get an idea of the upper bound. Having a tangible number of frequency in the vaccinated pop and the base rate would give a clear idea of what a better step to take would have been (i.e. not stopping vaccinations). I suspect a warning of the risk would have sufficed, if the rates even warrant this.
Pingback: Ask for a Dull Blade. | Placebo Parachute
Glancing quickly at the numbers, it looks as though pausing J&J would be worth it as long as it doesn’t delay vaccinations by more than 1 minute.
Zvi, did you make any updates to your personal ranking of vaccines in the last month or two? Is it still Pfizer > Moderna > J&J > Novavax > AZ > Sputnik >>> Sinovax for every age/sex/health condition? Is this ranking mostly based on the effectiveness against the variants that will (continue to) dominate in the next 12 months?
There are lots of cases and deaths in my current location, and people have a semi-serious approach to preventative measures, so I’m self-isolating till it’s safer to get vaccinated.
That’s still my rankings, although I think I’ve always had J&J roughly equal to Novavax if it ever matters. Does’t matter who you are. Pfizer>Moderna because of reduced side effects day after, equal effectiveness.
That last sentence hopefully means until you can get access, rather than till it’s safer to get vaccinated. It’s safe now, if you can get access.
I think he meant it was too risky to be in a place with other people getting the vaccine, because they might be asymptomatic infected, not that he would turn down a nurse coming to his house and jabbing.
From what I have seen, not getting vaccinated to avoid the one-time interaction is not a sensible level of precaution unless you happen not to want to ever be near another human being for the next six months otherwise, or something.
Do you have any thoughts or advice for vaccinated parents of young children? We want to resume living our less restricted lives but struggle comparing the direct risks to children and indirect risks of participating in transmission against continued limits on activities.
Young children shouldn’t worry you or cause you to limit your activity. If risks that low caused you to do that you’d never leave the house.
*You* should be safe leaving the house. Your *children*, on the other hand, who are not vaccinated, should not be interacting with other unvaccinated children, or at most with a small “bubble”; their lives *should* continue to be restricted until they can get vaccinated.
If your children are only exposed to vaccinated people, they’ll be fine.
Can you explain your reasoning here? If we look at the age dependence of IFR (see e.g. https://pubmed.ncbi.nlm.nih.gov/33289900/) then it is quite plausible that unvaccinated children might be less at risk from COVID than vaccinated adults. If the adults with whom they interact are all vaccinated, then why do their lives need to be restricted?
At what point is simple corruption a stronger hypothesis to explain vaccine pauses than tortured attempts to explain FDA psychology? Seems like a lot of smart people are being drawn into a convoluted game of speculation and not considering some more basic possibilities.
It’s always possible, but I don’t think we need that explanation nor do I think it fits the data. We’re a long way from there. If anything, actual corruption would be a relief here.
Zvi, don’t waste your caps lock key. Public health authorities know that everything you say is true. The problem: they have a strong incentive to act *against* the public interest. Simple: if you get J&J and you die from a clot, the health authorities’ backsides are on the line. If they pause and you can’t get vaccinated because of that, and you catch covid and die or get damaged, why, it’s clearly your own fault! No health authorities were harmed in the unfortunate case of your expiration.
And of course it can happen here. Had the US approved AstraZeneca, like almost every single country in the world, it would have happened a long time ago.
At one point I typed it out without the caps lock, looked at it, said ‘nope, that doesn’t sound right, it’s dishonest’ and went with the all caps.
You made the right decision. All caps have their time and place as ammunition of last resort.
Btw, I read your blog for weeks before I realized you are *the* Zvi of M:TG fame. Congratulations on your lifetime achievement!
Thanks!
To be fair, there exist other takes from the Post: https://www.washingtonpost.com/opinions/the-problem-with-the-johnson-and-johnson-vaccine-pause/2021/04/13/03b23f0e-9c96-11eb-9d05-ae06f4529ece_story.html
Curious for your thoughts on this: https://cspicenter.org/blog/waronscience/the-british-variant-of-sars-cov-2-and-the-poverty-of-epidemiology/
The most interesting argument is that B117’s transmissibility advantage over the original Covid strain may have varied over time, and may now be as low as ~20% although it could also be as high as is usually claimed (very large uncertainties).
Author isn’t a credentialed statistician, but is very skilled at stats (see e.g. https://statmodeling.stat.columbia.edu/2020/12/25/flaxman-et-al-respond-to-criticisms-of-their-estimates-of-effects-of-anti-coronavirus-policies/).
The J&J vaccine blood clot issue is headline news, but missing from the headlines or articles is how much worse is the incidence of blood clots vs. that from those who have had MRNA or PFE jab? From what i understand, those are not zero cases per million, but 4 or 5 out of a million vs. the 6.8 per million for JNJ.
Yes, and as mentioned above this is what should have happened with J&J, and the less said about this the better until the coast is clear.
The stumbling of our health authorities throughout this mess makes me think of Uriel. Not Uriel in his aspect as caretaker of the great machine. Uriel in Madrid.
I wonder if it might reduce the number of stupid decisions if we banned FDA people from watching the news. Or reading social media.
I’m not defending this decision, but I’ve seen a few people point out that many clinics are oversupplied with vaccines. The bottleneck in administration is increasingly becoming staffing, missed appointments, and just finding people who still both need and want the vaccine. If that’s true, then the J&J pause would have only a small effect on US vaccination. Of course, it’s still a mistake, but perhaps not a catastrophic one. They really should have just put a disclaimer for women of childbearing age and kept giving it to everyone else.
Also, how does one talk to vaccine conspiracy theorists. Asking for a friend. Is there any hope at all?
There are people who (at least before) were much more willing to get J&J than Pfizer/Moderna, or who were hard to reach in ways that made J&J a lot better, and this increased hesitancy on the other vaccines as well, so even if there’s still enough doses it’s pretty bad. I think we’re at a point where some places have enough doses and others aren’t there yet, but yes we should still be able to continue without too much percent damage – but even a little damage here is a lot of damage!
Three very relevant points from my extended-family Zoom call today, when we got into talking about Johnson & Johnson:
* My dad, a biostatistician who regularly works on new drug trials, considers the pause the only responsible option. Since there isn’t full FDA approval, he considers everyone taking the vaccine to effectively be part of a clinical trial, and pausing a clinical trial for weird side effects is The Done Thing until you know what’s going on. He didn’t bring up the public relations damage or the need for speed, and I didn’t want to press him in the group call.
* My cousin (herself vaccinated per her job in allied health) then said that her husband probably wouldn’t get vaccinated if he couldn’t get J&J. He really doesn’t want two shots, and he doesn’t want to wait a month nervously anticipating a second shot with worse side effects. Plus, he himself’s low risk for COVID. I’ve pressed my friends on similar issues, but she’s not someone I want to talk politically-adjacent issues with.
* Also, my cousin then said her state’s still only giving vaccines to people over age 65. I looked it up after the call; she’s two weeks out of date. I wonder how many more people like her are still needlessly waiting.
Hey Zvi, my family is getting vaccinated soon, and I was wondering if there’s anything I can do to minimize the infection risk at the vaccination point (besides using masks and gloves), as well as to ensure that the side effects won’t be so unpleasant. Any suggestions?
Also, how cautious should risk-averse people be two weeks after getting the second shot, in terms of washing groceries with a detergent, wearing masks in less crowded areas, going to shopping centers, using public transport, and having medical appointments? Only 20-40% of population in my country will have immunity by this time, and even if my family gets vaccinated, they will be still afraid of potential infection due to their age and health.
Nothing you wouldn’t be doing on other similar interactions – face away from people, wear the mask, gloves are marginal but sure why not I guess, keep your distance, etc etc. My experience was pretty good. As for the side effects, all you need to do is make sure you can crash for a day or two and use standard medication to mitigate and it’ll be fine.
I don’t think being afraid of infecting others once you’re vaccinated should change your life in substantial ways, but keep wearing the masks. At most, I’d stay out of highly crowded stuff.
The grocery thing was never actually necessary, and seriously, you can stop.
As a BC resident in their mid 40s it appears I could either get some AZ in the next day or two, or wait an unknown number of weeks/months to get Moderna/Pfizer. Our population is largely unvaccinated at this point, and we are on the verge of another surge in cases (and a corresponding lockdown, the most oppressive so far). Of course getting vaccinated won’t exempt me from the lockdown…
I’m curious what choice TheZvi would make in this situation.
If you can get AZ now for sure, or wait an indefinite amount of time, I’d take AZ now, especially with a potential surge coming.
Well, it’s not “indefinite” – the claim is that everyone will have a chance by July 1st. But that’s a long ways off.
Other factors
* might still end up with AZ even after waiting the longer period
* my family in aggregate has terrible OpSec and consequently we have an elevated exposure risk
I lean towards AZ but am feeling unexpectedly conflicted now the choice is upon me.
Get AZ ASAP and potentially get a mRNA later when supplies are plentiful. Unless you’re a female with almost literally zero covid risk over the next 2 months, and their tracking is good enough to deny you mRNA later, getting AZ is way better than waiting for mRNA.
Definitely this as well; once supplies are plentiful you can get the mRNA vaccine anyway (only one dose will be needed).
Nova Scotia here
The CBC is reporting possible issues with vaccine shipments, including AZ.
I wouldn’t trust predictions of future availability right now, and would grab what’s available.
(I’ve already had my first AZ shot – was just a little achy and lethargic the next day…no big deal)
If anybody can get “Abolish the FDA” shirts printed I will buy one.
Pingback: Covid 4/22: Crisis in India | Don't Worry About the Vase