
Omicron has fully taken over, and our uncertainty about it has mostly been resolved. The Omicron pandemic is now the Covid-19 pandemic, and we’re back in a kind of ‘normal mode’ albeit at the top of the Omicron wave.
A few weeks ago, the majority of the information and week’s discussion were in the Omicron posts. This week, the vast majority are in the normal weekly post, there’s only one pure Omicron post (although the Polymarket post was closely related) and it’s relatively short.
Going forward, after this week, my default plan is to incorporate the Omicron news and the Omicron-related predictions into the mainline weekly posts, and supplement with issue-specific posts rather than general Omicron updates.
If things continue to go well, I hope to use the resulting bandwidth to start doing less speed premium writing, and more longer term analysis, both on Covid and otherwise. There’s a lot I simply haven’t had the time to think about let alone write out properly.
Remember, this is a happy moment. We are no longer in (as much of) an emergency.
Severity
Thread updating what we know about severity of Omicron. Less severe in adults, less loss of taste and smell, mostly this is confirmation of the usual good news.
The issue of severity in children is less clear because Covid-19 is so non-severe in children it’s hard to tell the relative change.

All we know is there’s a lot more cases, and a lot more cases means a lot more child cases, and a lot more ‘with Covid’ cases means proportionally more child cases, and none of that is particular reason to doubt that the severity effect in children is different from that in adults, but we don’t know for sure because we lack the data, which results in for example the UK’s report saying about severity in children we have ‘low confidence.’ I agree that we are less confident here, but our baseline should mostly be that it roughly matches the adult changes, rather than a baseline of no change from Delta. But even if there is no change from Delta, that’s still not high risk.
Spread
BA.2 is the other sub-variant of Omicron, whereas BA.1 is the one that shows up on S-gene deletion tests and it most common in the USA and UK. This thread discusses whether we should worry about BA.2, and offers this chart, you can get more at this website.

If we take this at face value, it was 10% of Omicron cases on 21 December, and is about 30% of Omicron cases on 8 January, which is about two doublings in three weeks. Even with fast generations that edge is substantial, and is one reason to expect this to blunt downward trends somewhat, but the rates of decline of BA.1 are faster than this in places where BA.1 is declining, so this is unlikely to be additionally scary in those areas. If BA.2 ‘gets there first’ in a given area, it would lead to a higher peak, and it makes containment by China potentially that much harder.
Wastewater surveillance is available in a few places other than Boston so here’s some data from California.

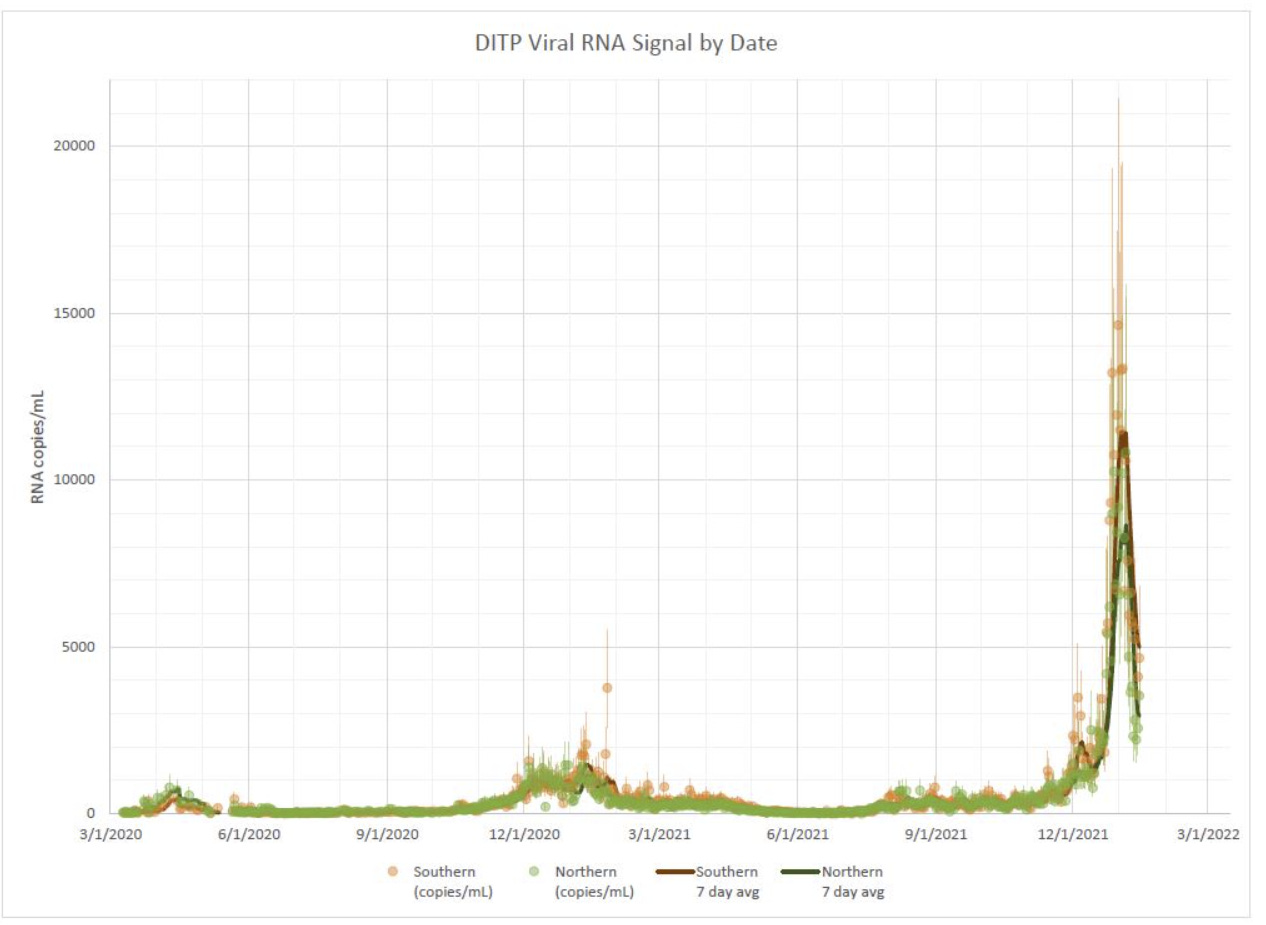
Whereas Boston continues to be a straight line rapidly dropping down (interesting note is that the ratio of north Boston to south Boston doesn’t seem very constant?), the California data represents a gentle peak that doesn’t seem to be continuing to drop, in a way that doesn’t have an obvious physical explanation. I’m not sure what to make of it.
A basic but well-executed thread from Bob Wachter that spells out how much Covid is out there right now, and thus how much less risky activity will soon become. The difference will be extreme, although I’m not convinced it will be quite this extreme.
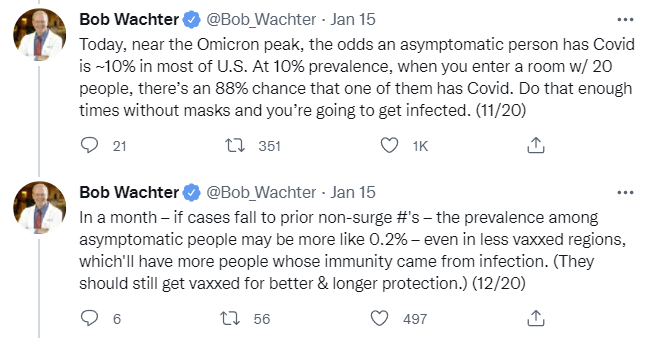
That’s a factor of 50, a 98% decline in relative risk of a given activity (e.g. microCovids), within a month. I’d be surprised if we get a 98% decline within a month, but I’d be highly unsurprised by 90%, and even more surprised by “only” 70% declines from peak (in actual infections) than I would be by 98%. We will never know the true number.
Some anecdata offered in the comments from an unmasked dance party.
As promised, Remolino policy towards COVID-19 will be full disclosure of all information. Therefore – there were 82 infections among a total of 509 Remolino participants.
Of those:
– 7 infections among 10 elves;
– 6 infections out of 21 DJs;
– 3 tests came positive from the lab out of 41 PCR and 145 antigen;
– 2065 self tests were distributed altogether;
– 12 people could not come to the festival because they got infected a week preceding or during the festival, and 4 people had Covid just before the festival, but came after recovering;
– 113 people canceled before or during the festival before arriving to Lviv, 7 people left earlier than registered for;
– of all infected, 62 had first positive test only after they arrived back home;
– among all participants, 11 have not had vaccine or confirmed previous infection;
– we have a confirmation of Omicron from at least one sequenced specimen
The NBA Covid index, which continues to be our most reliable, says we’ve peaked.
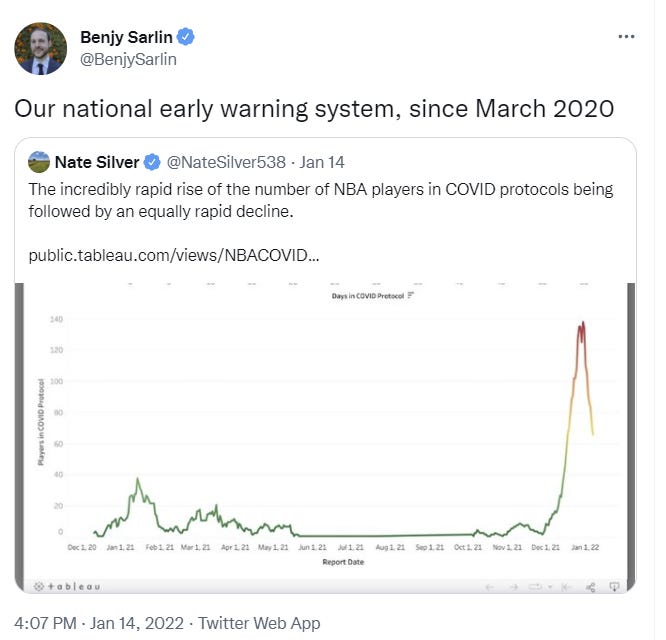
Note that it doesn’t mean we were already down by that much by the 14th, the NBA tends to be somewhat ahead of the curve so they’ll peak somewhat earlier, but you can tell how much earlier by looking at the graph.
Evidence from Japan says Omicron cases continue shedding virus for longer.
Scott Gottlieb is skeptical that China can contain Omicron, despite doing things like killing all the hamsters in Hong Kong.
Prediction Updates
China keeps daily cases under 50 per million through 2022: 30% (unchanged).
On the one hand, Gottlieb is skeptical, although it’s hard to translate that into his probability since he doesn’t talk in those terms. On the other hand, killing all the hamsters is a costly signal of seriousness, even if it’s not a very effective countermeasure. I’m roughly unchanged for now, and this is long enough term that the time lapse doesn’t carry much weight yet either.
Median peak cases day for United States: January 19 → January 15 (but only ~70% to have already happened, with most of the rest being later this week, if we’re going by measured cases, delisting but not evaluating yet)
Mode peak cases day for United States: January 19 → January 15 (delisting but not evaluating yet)
Daily cases in the the United States have peaked by February 1: 90% → 98% (delisting).
If we use OurWorldInData as our canonical source here, it looks like the peak already happened on January 15. That’s definitely the mode day. The question is whether the holiday backlog will cause us to bump above it before heading back down. Week over week cases (from Jan 13 to Jan 20) are looking very close to flat on Wikipedia chart, which is consistent with a mid-week peak.
Either way, the peak in reality (without removing lag times) was sometime between January 15 and January 20, which means with lag times it was several days before that. Delisting and evaluating the peak in January to true, will evaluate the mode and median as soon as we know the exact date but not going to update them further.
Will There Be a Federal Mask Requirement on Domestic Flights as of November 8, 2022? 45% → 44%.
There’s a market now at Polymarket, and it’s now at 43% so adjusting slightly.
Chance that Omicron has a 100% or bigger transmission advantage in practice versus Delta: 45% (unchanged).
I’m considering this to be about BA.1 rather than BA.2 and I still think the math is close. I’m going to stop updating it unless we learn more, because I don’t expect us to ever truly know, and conclude that it’s something relatively close to this.
Chance that Omicron is importantly (25%+ in the same person) less virulent than Delta: 97% → 98% (delisting).
Evidence keeps piling up, suspending this prediction unless number goes down and evaluating to true, leaving the 2% for model error.
Chance that Omicron is vastly (75%+ in the same person) less virulent than Delta: 30% → 40%.
The death numbers in the United States are not going up. There’s all these reports of hospital cases not matching the paths we see in Europe, but the death number this week looks like it’s not going to have gone up. It’s going to be about the same, causing my prediction to miss, and I need to adjust for that.
Chance we will be getting boosters modified for Omicron within 6 months of our previous booster shot: 20% → 15%.
Chance we are broadly looking at a future crisis situation with widely overwhelmed American hospitals, new large American lockdowns and things like that: 2% → 1% (delisting).
Omicron is already on the decline, or at worst will be on the decline within the week. By the time the boosters arrive in March, I don’t see any reason to be pushing an additional booster on anyone who was already recently boosted outside of the highest-risk groups, and I don’t consider that to count on its own, but our elites can get crazy about such things, so I can’t fully rule it out and there’s no market.
On the crisis, the answer is no, not unless something crazy and highly unexpected happens, and most of the crisis situations that happen in 2022 are caused by things other than Omicron. I’m delisting and evaluating to false.
That’s a lot of delisting probabilities. I plan to add some of the Polymarket markets to replace them, but I already dealt with that on Monday, so not going to duplicate it now since little has changed since then.
Suggestions for additional markets and predictions are always welcome.

The NYT seems to agree with you, as per their headline story in their newsletter this morning.
Some news on the China front:
https://www.cbc.ca/sports/beijing-reports-first-local-omicron-case-ahead-of-olympics-1.6316792
I also saw an article in the past few days, although unfortunately I can’t find it now, saying China was cranking up PCR cycle counts to 40 instead of the usual ~30 in an effort to increase sensitivity and catch every possible case.
Zvi, given the current data, is omicron more like ~50% or ~90% less dangerous than delta? Also, in the absence of Paxlovid, would you combine Fluvoxamine with budesonide or something else (or take it alone)?
I answer the first question directly in the predictions section. Budesonide I continue to not have investigated yet. I would take Fluvoxamine if I have access to it.
Zvi, why aren’t the P100 masks commonly recommended in public health campaigns? They are way more effective than surgical and N95 masks (3-10x more), more comfortable than N95s, better for the environment, harder to contaminate while touching the outer side, and cheaper in the long run. In retrospect, wearing anything else seems kind of… silly?
Also, how long should one set of filters in such a mask last (while offering a high degree of protection against omicron)?
P100s are not recommended because they don’t think public and/or production lines can handle it. Whether they’re right or not is beside the point. I endorse them.
No idea on filter survival.
Filters in those masks work more or less forever. The only reason to get rid of them is they get clogged, so become harder to breathe through, but filtering efficiency actually increases with time. That’s not covid specific, but from the guidelines of use in various dirty production environments.
They’re more comfortable partially because the air you breathe out is not restricted. There’s a valve, not a filter. Masks have most effect when worn by the infectious person. So it’s a good mask from a personal point of view, but from a public health point of view it’s bad.
If you’re wearing a p100 you’re probably being careful enough in general that you’re no threat to anyone.
On the public health question, it’s a bit funny because insofar as other masks work it’s a pretty small effect. Preventing yourself from getting infected is a great way to avoid transmission. If everyone used a p100, there would be basically no transmission.
Also, high risk people could use them and then low risk people wouldn’t have to wear masks.
No. Some elastomerics have outlet valves. Some don’t.
While I understand the desire to use long words, p100 and elastomerics are not fancy synonyms. And while elastomerics, indeed, have recently been made without valves, nobody in their right mind will wear them for covid, because they are extremely uncomfortable. Regular p100 masks are not made without valves to my knowledge.
Because it’s demented to wear a freaking respirator mask for the rest of your life to avoid the sniffles. Listen to yourself, man!
Only just in the past two weeks did we have any positive cases among the kids at my daughter’s daycare (only parents and teachers). We went from zero known cases in a year to half the classrooms closed because of known cases. Lack of testing may play a role, but even if the kids were getting infected they obviously weren’t passing it on to parents and teachers in any great quantity, and we DID test our daughter several times when she got a cold/the flu, whatever. (All three of us wound up testing positive with light symptoms, but our unvaccinated 3-year-old was even less affected than her double vaxxed and boosted parents.)
Do the S and N lines on the CA wastewater graphs refer to the amount of S-gene vs no-S-gene material in the wastewater?
If so, how are these compatible with omicron being dominant??
I am also confused by this. I believe https://soe-wbe-pilot.wl.r.appspot.com/charts#page=overview is another presentation of the same data and it has a del 143-145 line which I believe is omicron.
So odd to me that American death rates have not jumped whereas Canada’s certainly have. Wonder the cause behind that.
The fact that that’s happening in Canada is mysterious indeed. I hadn’t seen that.
Base rate effect. Canadian deaths were very low pre-omicorn, while in the US, delta wave was in full swing.
Just spitballing, but Canada’s vaccination rate has broadly been higher than in the US, and Canada has enjoyed more universal implementation of, and cooperation with, NPIs. Through previous waves this may have led to fewer people who were susceptible to severe outcomes becoming infected in the first place. In terms of deaths per million residents, Canada has had less than 1/3 the death rate of the US. Presumably some fraction of that 2/3 who might have otherwise died, but haven’t so far, remains susceptible and they are much less able to avoid infection with this time around. Something of a regression to mean in Canada, and a survivorship bias in the US. .
That said, muddying it all further, the current death rate in Canada is still significantly lower than in the US. The low point in the 7 day moving average US daily death rate in the past 5 months was November 7 with 904 deaths, or ~2.69/million, and it recently peaked on January 15 at 1886 or ~5.65/million and currently sits at ~5.07/million. In Canada, deaths were stable at about 20 per day through November and most of December, or ~0.52/million, and it is currently at 124 per day, or ~3.24/million. So indeed the growth in the death rate has been more significant in Canada through the Omicron wave, but Canada started the wave with a dramatically lower (1/5th) ongoing rate of death and even with catching up rapidly, it has not yet caught all the way up to the US (US rate still >1.5x higher). I expect Canada is soon approaching its peak of deaths for this wave, and I give it a fair chance of remaining below the US rate throughout.
There’s been some interesting paxlovid news over the last couple days:
(1) The speedy development of paxlovid was in large part due to serendipity: Pfizer already had a candidate 3CLpro inhibitor for the original SARS in 2003, so they got the world’s best head start. That’s serendipity on steroids, so congrats to the Pfizer team for jumping on a good thing when they saw it.
(2) A bunch of studies have dropped on bioRχiv_ (as pointed out by a Pfizer press release, of course), showing paxlovid retains good efficacy against the Omicron variant. It has a Ki of about 1nM against the target protein in all variants, and an EC50 of about 20nM, so it’s very potent indeed. The EC50 for reduced viral load might even be better in Omicron than the original strain. Also, the IC50, where you get actual 50% inhibition, appears to be comparable between Omicron and the original strain.
All pretty good news, no?
The continued assumption of independence when assessing COVID risk in a group is annoying. If the prevalence is 10%, it is *very* unlikely that the people in the room with you all have an independent 10% chance of having COVID, except for rare circumstances (say jury duty). So the actual risk of having a COVID-positive person in such a room of 20 people is likely to be either >> 88% or << 88%, and you can probably use demographic or other behavioral information to figure out which side of that distribution you are on at that moment, albeit with substantial uncertainty.
I think the slow decline in Santa Clara County can be explained by a high tolerance for NPIs. In the face of something as infectious as Omicron, that doesn’t avoid people getting infected, but it does stretch it out.
Suggestion for additional (long-term) market: >= 70,000 US COVID deaths between December 1, 2022 and March 31, 2023 (inclusive).
Reference points: between 2010/11-2018/19, CDC estimates for US flu deaths average to 35K/year; this looks to be >90% concentrated in the indicated interval. Current pace for the same time period would put the number at roughly 160K; it was ~260K last winter (all data from OWID). The daily US deaths data for 2020/21 and 2021/22 look remarkably similar in shape so far (but obviously are different in scale; maybe this pushes the estimate for this winter down to 145-150K.
Relevant questions and [guesses]:
1. Will there be deadlier or more-escaping variants in 2022? [Weak yes.]
2. Will boosters be readily available? Will population-wide discipline in getting boosted match current rates? [Weak yes. No.]
3. Will testing be more available? Will the population strata where COVID kills be less likely than average (or less likely than now) to use testing? [Weak no. Hard yes.]
4. Will paxlovid (or molnupiravir if it’s effective and safe and approved) be available in sufficient quantities, especially if there are relatively few summer COVID deaths? Will the population strata where COVID kills be likely to seek treatment quickly enough for paxlovid to help? [Weak yes. Weak no.]
5. Will we have multivalent boosters? Will we have data (along the lines of flu surveillance) from the rest of the world that lets us choose the composition of multivalent vaccines more effectively? [Weak yes. Weak no.]
I’m not sure how I feel about my 70K number. I’d definitely buy at 40K, and I’d definitely sell at 150K (maybe hedging such a sale via buying S&P puts and VIX).
Thoughts?