
Omicron is now the dominant strain, so much of what would otherwise have gone into this Omicron post ended up in the latest weekly post instead, and I’m considering the right way to merge the two streams together.
In addition to some amount of the usual business, the focus of this post will be an explicit attempt to look at what’s likely to happen from here, and give my baseline scenario.
I recently had reason to chart out what I expected that baseline scenario to be around the world, so it makes sense to share it here.
The world can be divided into five (highly unequally sized) parts, with increasing levels of uncertainty, some places are unclear on whether they’re in groups two, three or four:
- South Africa and other already-peaked areas.
- Uncontrolled spread: Europe, North America, India, Israel, Australia and Argentina.
- Without an Omicron wave, or without good data: Third world, Russia.
- Previous containment: South Korea, Japan, Taiwan and New Zealand.
- Special case of previous containment: China.
South Africa and Other Already-Peaked Areas
This is the easy story to tell. Predictions about the past are often still hard, but they’re a lot easier.
A few African countries have already finished their Omicron waves, and got through mostly unscathed. Since they’re in the southern hemisphere, one can worry that there’s a wave coming in their winter a few months from now, but I would expect any such wave to be mild even if relatively little is done to prepare, given how things went this time, and that those infections are now baked in.
Uncontrolled spread: Europe, North America, India, Israel, Australia and Argentina.
This is where most of my readers live, and where I live, so it’s been my main focus. There is now a very clear baseline scenario.
Infection rates increase exponentially until they hit a peak. In major cities, this plateau will usually be quite high, with more than 1% of people infected each day, and likely 10%+ of the population testing positive at any given time. In rural areas, the plateau is likely going to be somewhat lower, but not dramatically lower.
Once you hit that peak, there will be a short period (a week or less probably in most cases) before the decline starts in earnest, then picks up speed. Once it’s gone down to something that will usually be between 25% and 50% of its maximum over the course of a few weeks, the decline starts to slow in percentage terms as behaviors adjust back somewhat. Then over time, there is a slow decline, which mostly continues until such time as other dynamics (like weather, or another variant) change the game once more, or you stabilize at low endemic levels.
There are substantial disruptions during the peak period, lasting roughly a month, but nothing as scary or severe as early 2020, and no breakdowns of civil order. Schools end up closed for a few weeks to a month in many places, others have to quickly close for a few days due to staffing issues, but some manage to stay open and it’s fine, they don’t meaningfully make anything worse.
As long as the hospitals manage to continue to provide care, there’s a ton of cases, but not that many deaths. The hospitals come under stress about six days after the relevant cases, through a mix of a lack of staffing and a flood of new patients. The question is what the true capacity is, and what happens when you exceed it, and what our ability is to do triage. Even when we ‘get through’ those weeks, life in the hospitals is still terrible during this period.
Once hospital admissions peak and start turning downward again, and it’s clear this isn’t simply hitting capacity limits and turning people away, we can know that we’re going to make it through in a given area.
We do know that London and New York in particular are almost certainly going to be fine, but other areas have lower capacity, sometimes much lower, and are ‘running behind’ in terms of how far along on this map they are, so they are not yet in the clear.
One can talk in terms of countries, but the situation is everywhere a local phenomenon.
Even within New York City, Manhattan has peaked, Brooklyn probably peaked a few days after that, but the rest of the city probably hasn’t peaked quite yet. I don’t know the details in London, but the situation is likely similar, with the center already declining, but other areas still going up along with the rest of the UK. The combining of local peaks into a region or nation gives a broader curve that looks less dramatic than the local graphs.
Who gets there when?
New York and London (or at least their central areas, and their aggregates) are the two places we can confirm have already hit peak. San Francisco has the hospital data that shows something similar, so it’s likely many major cities are also in this group.
Most other places are running somewhat behind that. The more rural you are, the slower things are to develop, and the decline will likely also be somewhat (although not as much) slower.
A lot of Europe and North America are on remarkably similar timelines. The United States, United Kingdom, France, Spain and Italy are all in this group.
I expect the peak for this group to be something like January 19. Exponential growth happens fast, so there’s less uncertainty in the timeline than there might appear to be, but being a week off in either direction would still be inside my 80% confidence interval. If the group hasn’t broadly peaked by month’s end, that would be very surprising.
Other places got started slower, but are still in the same boat. This is a combination of less international travel causing things to start slower, and slower spread once things get started. If there’s a place that has a lot of travel but hasn’t taken off yet, it’s probably developing slower, and its timeline will get further behind over time. Whereas places that have less travel are likely equally fast.
Here’s some of the key members of the group.
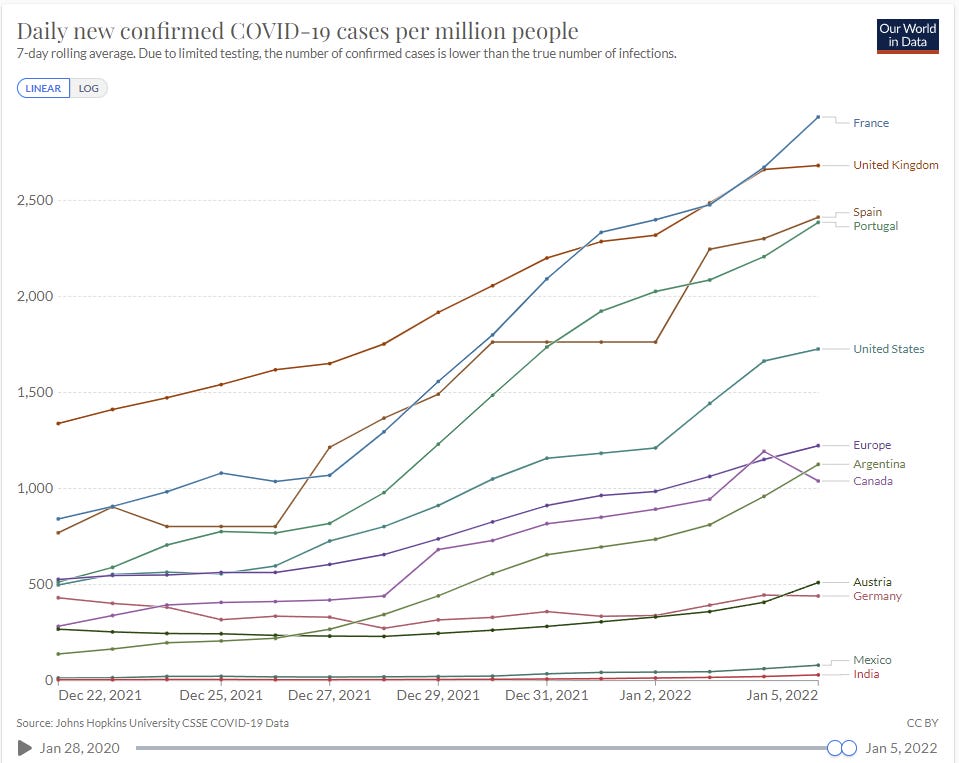
And here’s only the ones that have low case numbers.
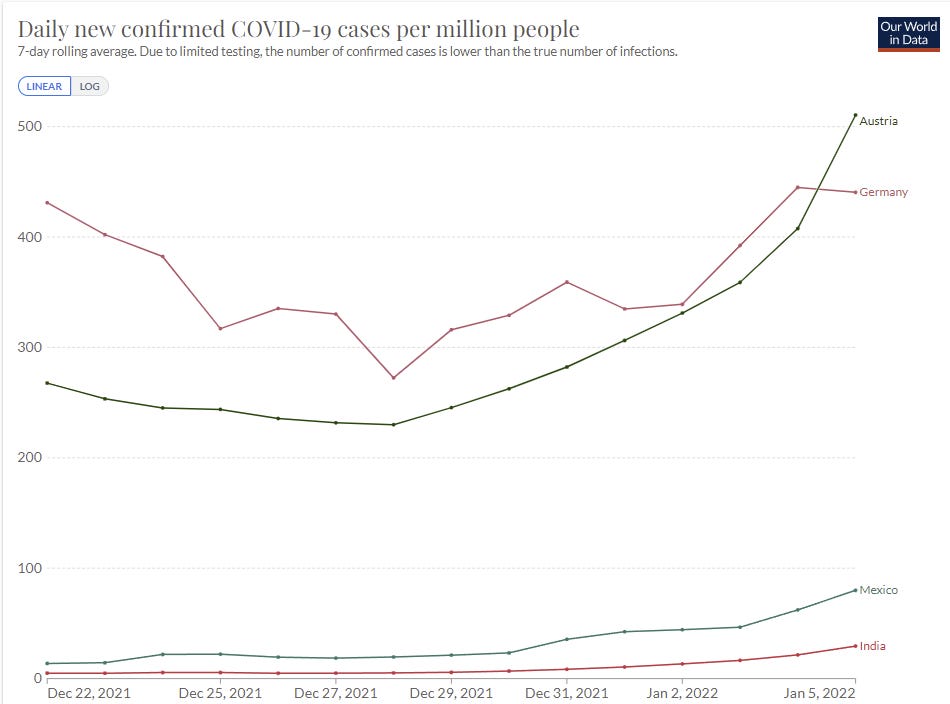
Austria, Mexico and India here all show accelerating growth as Omicron takes over from Delta. Germany is the weird one, where there’s been sufficient prevention to make it close, but looking at the Omicron-specific graphs makes it clear that the same thing is going to happen eventually, it’s simply going to happen slower, and that extra time seems unlikely to be put to good use. There won’t be that much of it. I’m still confident they belong in this category.
Canada is doing a more reasonable thing, and instituting prevention measures when they get in danger of exceeding their hospital capacity, to try and flatten the top of the curve. Flattening the curve on the way up doesn’t accomplish anything, you need to flatten the top. I don’t expect it to accomplish all that much or be worth the trouble, but at least it’s not automatically doomed. The last day of data is likely a reporting delay there.
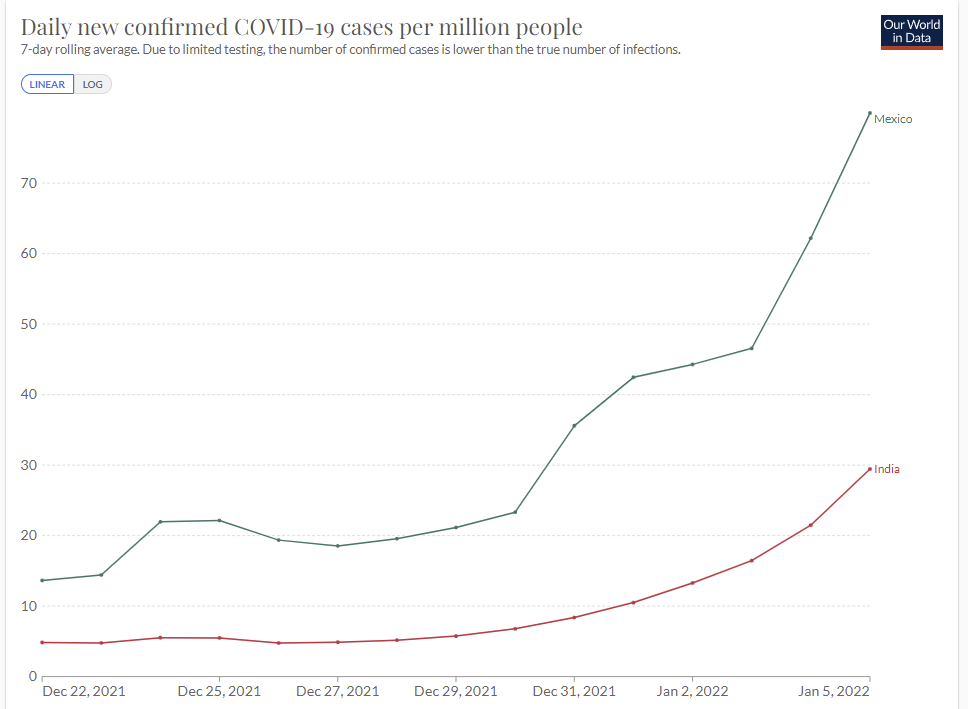
Mexico and India are a few weeks behind the USA and Europe, but they’ll get there soon enough. Note that deaths in India have been severely undercounted. When things get bad in India, that is the place I am most worried will get quite bad, and we should be thinking now about how to use aid to get mitigation efforts in place.
The fundamental insight is, either you can contain this thing, or you can’t. For a while Mexico didn’t look like it had a problem, but there was no reason to think they could contain it, so all that did was delay things. India was the same, and now we are seeing the same rapid exponential growth there we saw elsewhere, and getting to 1000+ from 30 is not that many doublings. They’re only two or three weeks behind.
There are doubtless some places I’m missing here. For example, when I started writing up the model Peru wouldn’t have been included, but it probably goes here now, and Brazil could join soon as well.
Without an Omicron wave, or without good data: Third world, Russia.
Some such countries show some signs of a potential wave, but many flat out don’t, as you can see here.
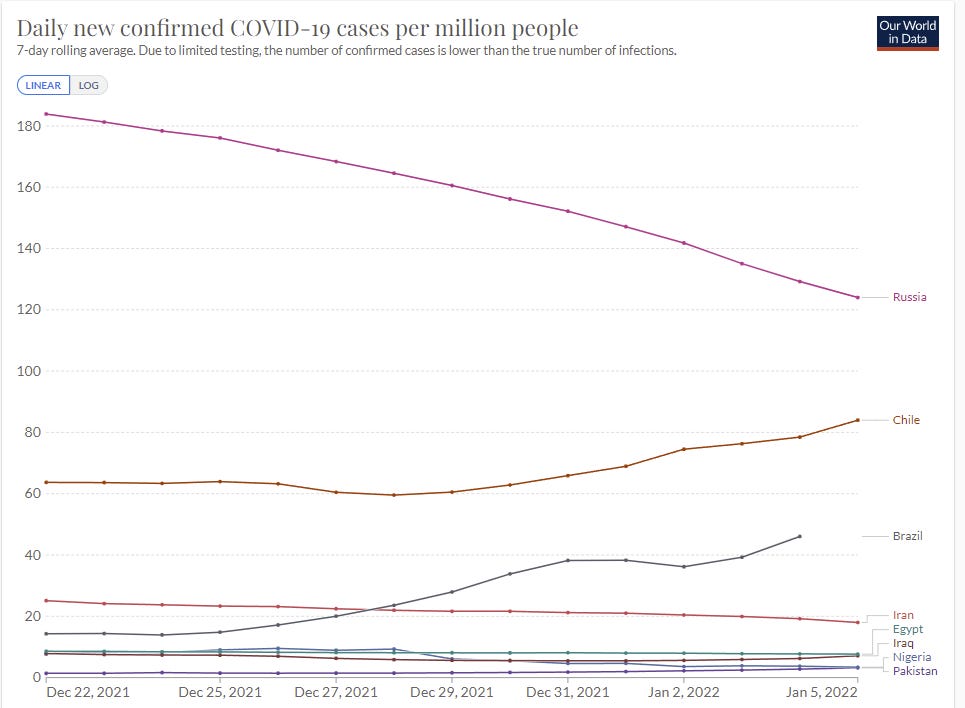
Many of these places have had much higher rates in the past, so it isn’t a pure testing issue for them. Some of these places are sufficiently unnatural places for Covid-19, at least at this time, that it’s possible waves will not arrive, or that once they get to moderate levels moderate behavioral adjustments will stabilize things at a level they can handle.
The key distinction between this and the next category is that these nations didn’t take extreme measures to get containment, which gives potential for more slack to solve the issue or contain the damage.
Previous containment: South Korea, Japan, Taiwan and New Zealand
If Australia was on the graph it would destroy the y-axis. That’s what happens when procedures that previously were sufficient become inadequate. Here South Korea is still doing a similar thing, levels are very different.
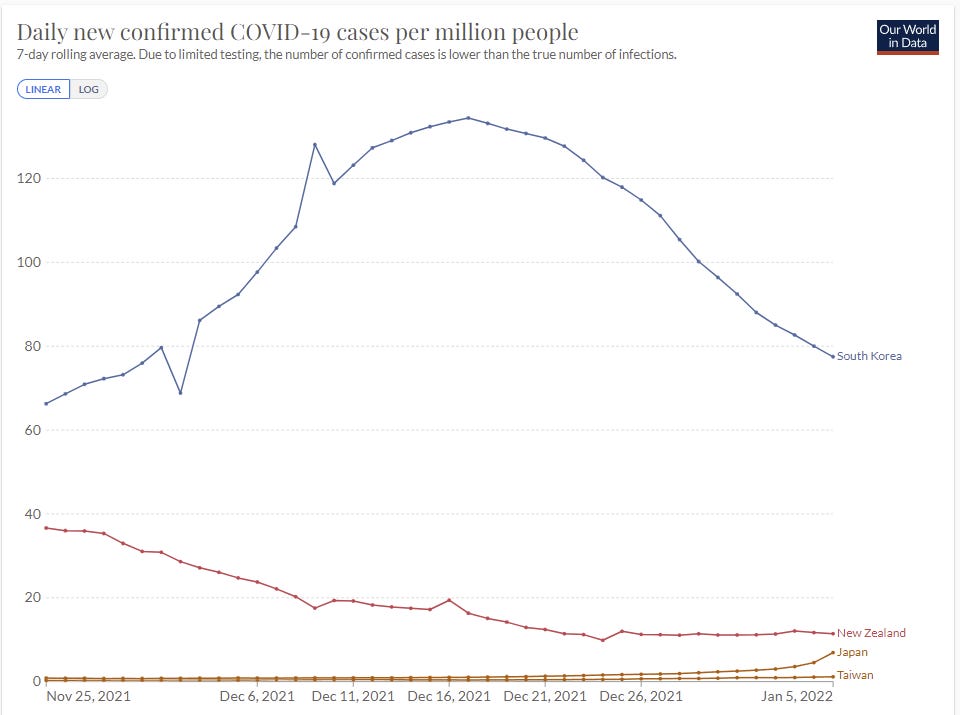
Word from New Zealand in the comments is that border controls are holding for now, but that this is widely expected to fail, and if Delta wasn’t fully wiped out then I agree with this assessment. It may be a bit, but they’re going to be in group one before their winter is out.
The last few days in Japan do not bode well, but it’s probably fine? They’ve gone from under 1.66 per million two weeks ago to 6.91. That’s one doubling per week. My guess is that Japan retains enough slack to continue to contain the situation. Taiwan also seems like it’s got a chance.
For now South Korea is still headed downwards, which indicates they’ve managed to keep Omicron out, but also they got high enough before that I am highly skeptical that they can contain this for that long. I expect them to end up in the first category.
That leaves the big one. China.
China
China is the big question. They managed to maintain a zero Covid policy so far, so almost none of them have immunity that way. The Chinese vaccine was always less effective, and offers minimal protection against infection by Omicron.
Thus, China is facing a much harder problem with Omicron than they faced in previous waves. Measures that previously would have been enough will no longer be enough.
Locking down Xi’an, with 1% of their population, has been frustratingly slow at containing the situation there. My presumption is that China can and if necessary would continue to do things on this level, but that doing that for 10% of the population for long periods is a very different proposition. There is only so much ammunition available.
Thing is, if China can’t get to and stay at actual zero Omicron, then they need a sustainable way to keep it from exploding, or they will lose and nothing they do will matter. Taking extreme measures on outbreaks requires that the rest of your strategy be close to enough on its own. Keeping things out via borders requires that you really mean it, or all you do is slow things down.
Meanwhile, they’re planning to host the Olympic Games, and, well, whoops?
I’ve underestimated China’s containment abilities throughout, and been repeatedly surprised. Once again, I’m skeptical they can pull this off, and once again it’s mostly a Boolean, either the strategy works or it doesn’t. But given their track record I can’t count them out of it, neither result would surprise me, nor could I find any prediction markets that speak directly to this. Where there is a will, there can sometimes be a way, and China has a will in a way that Western countries do not.
I’m going to tentatively put my probability that China keeps Omicron contained at 40%, but I don’t have great knowledge about many details that could update that, including the opinions of others who have thought about it. So I would update quickly, especially if someone offered to wager on either side.
Now a round up of the other Omicron News. Remember, a lot of this got moved to the weekly update.
Vaccine Effectiveness
Third dose holds up at 90% effectiveness against hospitalization for at least three months for the elderly. UK using this to decline to authorize fourth doses.
In this study, we demonstrate both markedly decreased neutralization in serology assays and real-world vaccine effectiveness in recipients of two doses of vaccine, with efficacy partially recovered by a third mRNA booster dose. We also show that immunity from natural infection (without vaccination) is more protective than two doses of vaccine but inferior to three doses. Finally, we demonstrate fundamental changes in the Omicron entry process in vitro, towards TMPRSS2-independent fusion, representing a major shift in the replication properties of SARS-CoV-2. Overall, these findings underlie rapid global transmission and may alter the clinical severity of disease associated with the Omicron variant.
…
Our estimates of protection in the current GG&C cohort, whose median time since most recent dose is 5 months, were notably lower (Fig.4D). This waning of protection was evident for both variants, leading to very low levels of protection against Omicron in double vaccine recipients of ChAdOx1, BNT162b2 and mRNA-1273 (5.19%, 24.39% and 24.86% respectively). Our estimates for current protection against Omicron in recipients of a third booster dose of BNT162b2 or mRNA-1273 were much higher at 59.21% and 64.9%. We next estimated the additive protective effect of previous natural infection. Infection-acquired immunity directed against other VOCs may be broader in nature and may wane more slowly than that induced by vaccines. The level of protection following previous infection was 53.2% for Omicron, and 88.7% for Delta.
Paper has a bunch more detail along with some cool diagrams and charts. These numbers all make intuitive sense to me.
Meanwhile, vaccines in children are ludicrously effective in terms of reducing what risk is left, a 180x reduction, although they are also largely unnecessary in terms of the kids not having been at much risk in the first place.
Testing
‘Ethical rules’ versus the need to f*** around and find out. We are all poorer for it. We should be able to have very good info on relative performance of different tests, in particular. Here’s some new results, which suggest that nasal swabs are slow to start turning positive, in the study median additional time required was 3 days after the PCRs were positive, which is in the range of not being all that useful if you need to confirm you’re not infectious. Suggestion is to use saliva for rapid tests to get that time back, but by the time we do that, I’m assuming the wave will already be over.
Combined with a lot of anecdotal reports I’ve seen, I’m moving towards assuming that while rapid tests are probabilistically very useful, transmission with Omicron is much faster and has outpaced the speed at which the tests turn positive, and this means that if you want to be confident rapid tests are not that useful on their own. And strongly agree with Mina that if you have symptoms, you have to act as if you’re positive unless you’re negative several days later.
As it usually goes when we are scared of public reaction and use price controls rather than ration to those who value something the most, here is the ongoing quest for Binex tests.
Hospitals
Report of hospital telling employees to return five days after first symptoms or positive test unless they have ‘true Covid symptoms,’ and otherwise being forced to work while sick, including with those true Covid symptoms.
Hospitals in DC risk being overwhelmed and going into crisis care mode, but have seen few deaths. They’re bringing back Covid-positive staff quickly, and offering increasingly rich shift bonuses of $1000 or more.
Hospital admission growth rates in UK, London has gone negative and we are clearly past peak growth. The danger is always that if you get close to the edge you start turning people away and then the graph is misleading you.

Report from NHS, seems consistent with previous reports.
Threads and Posts
Your Local Epidemiologist brings us the good news, general summary post. All seems right, good summary, nothing new.
Look at the impact of Omicron on cancer treatment.
Eric Topol breaks down the details of why our immune systems have been dealing with Omicron so well.
An argument moderately against Omicron coming from Gain of Function research, including what new information would move the needle.
WHO being an unhelpful broken record.
Probability Updates
I want to explicitly encourage people to say in the comments which predictions you disagree with, what your probability is, and what your model is that is causing you to disagree. Especially on China.
China keeps daily cases under 50 per million through 2022: ?% → 40%.
I talked about this above, and expect to update this soon more on better thinking and others’ opinions (including prediction markets if we can get one) rather than primarily through new information. We’ll know if this is failing, but in most worlds where this fails it doesn’t fail right away, so short term lack of evidence of failure is only weak evidence of long term success. I’m mostly throwing this out to start a conversation.
Median peak cases day for United States: ??? → January 19, 2022
Mode peak cases day for United States: ??? → January 19, 2022
Daily cases in the the United States have peaked by February 1, 2022: 85% → 90%.
I think this is better than more probability estimates here. Note that the most likely path is that the median updates to somewhat later as we continue to see case growth, rather than me expecting the peak to be the next day as a median and then the next day we get a peak, we get an asymmetrical distribution. The mode is more likely to stay where it is or not move much, and will likely quickly become ‘any day now’ if it doesn’t happen when I expect.
With some areas already peaking we can be more confident the peak will come in January, but not super confident until we see it in more places more definitively. There’s still a lot of error bars.
Will There Be a Federal Mask Requirement on Domestic Flights as of November 8, 2022? 50% (unchanged, no new information).
Chance that Omicron has a 100% or bigger transmission advantage in practice versus Delta: 55% (unchanged, no new information).
Chance that Omicron is importantly (25%+ in the same person) less virulent than Delta: 90% → 95%.
Chance that Omicron is vastly (75%+ in the same person) less virulent than Delta: 25% → 30%.
Time keeps passing and we keep seeing the same patterns, I think we can safely say that it’s importantly less virulent, I’m keeping the 5% around mainly for model error (e.g. maybe my reasoning is bad). I’m up to 30% on there being a big difference based on the large disconnects in deaths, including in the United States.
Chance we will be getting boosters modified for Omicron within 6 months of our previous booster shot: 20% (unchanged, no new info)
Chance we are broadly looking at a future crisis situation with widely overwhelmed American hospitals, new large American lockdowns and things like that: 5% → 3%.
The big cities, especially the blue ones, are going to get through this, and I don’t see any way big lockdowns happen based on the needs of rural areas.
Generation time (serial interval) of Omicron is 3.5 days or less: 87% → 90%.
Creeping up a bit on reflection and on everything continuing to fit the pattern, especially the reports of rapid tests not picking up on the newly quickly infectious. Pretty confident here at this point, but don’t know we’ll ever confirm this.

> Chance that Omicron is importantly (25%+ in the same person) less virulent than Delta: 90% → 95%.
> Chance that Omicron is vastly (75%+ in the same person) less virulent than Delta: 25% → 30%.
One thing I’ve seen little mentioned is Omicron severity vs. the original strain. My impression is that 25% less than Delta is still worse than original, but 75% less than Delta would be better than the original, but I haven’t tried to pull detailed information on this or done the math. Do you (or anyone here) have good info on that benchmark?
It’s weird to me that we’re consistently saying “It’s less severe than Delta” and only once have I seen anyone say “but that still likely worse than the original”, and I suspect it’s unintentionally mislead a *lot* of people into underestimating the severity.
If that were the case, is this not finally a case of misleading to get people closer to the truth?
People that weren’t familiar with the stats, particularly for under-60 healthy people, had the impression of a much higher rate of danger for the original strain than it really had. If they’re going to continue not to look at the stats, authorities saying things that have the emotive meaning “the current situation is safer than what you’ve been worried about” seems like the way to get their models closer to reality, even if there’s a bit of semidishonest handwaving about what it was particularly they had been worried about.
Some people over-estimate the risk, but there’s no shortage of people vastly underestimating it either.
At any rate, this seems argument pretty akin to the various noble lies leaders committed early on. I’d like us to try truths for a while.
I would too, but maybe the “finally” was too subtle.
Is Delta in fact worse than the original? I thought I read somebody (maybe even Zvi?) saying that, like Omicron (only to a lesser degree) it was more contagious but less virulent. Maybe that was just relative to Alpha or Beta?
I’m not 100% on this.
A quick Google search mostly suggests it yes, but I did see this study finding otherwise: https://jamanetwork.com/journals/jama/fullarticle/2787105
The only thing I found from Zvi was that Delta is more “deadly” (separate from the infection rate) but I feel like it’s from early enough in Delta’s spread that the data could easily have shifted: https://thezvi.wordpress.com/2021/07/15/covid-7-15-rates-of-change/
That post also links to https://unchartedterritories.tomaspueyo.com/p/delta-variant-everything-you-need which provides a “it’s more deadly” source of https://www.medrxiv.org/content/10.1101/2021.07.05.21260050v1
We’ve all essentially calibrated to Delta at this point, so I figured this was the best comparison. I do think ‘back to original strain’ was my baseline for a while, but I now expect somewhat milder than that based on outcomes.
The study demonstrating a higher level of protection (~2x) for previous infection than previous two-dose vaccination goes a long way toward explaining the stubborn persistence of higher case rates in the vaccinated cohort than the unvaccinated.
I am starting to see signal now that even in non-urban areas the higher case rate among the vaccinated is persisting. We have data from British Columbia, Canada current to January 3 that breaks down case rate to regional health authority. This data is available here, on the “Outcomes by Vax2” tab: http://www.bccdc.ca/health-professionals/data-reports/covid-19-surveillance-dashboard
BC Overall Case Rates: Jan 3
Two-dose: 72.5/100k
Unvaccinated: 49.7/100k
One-dose: 37.1/100k
Three-dose: 32.0/100k
Vancouver Coastal (Urban):
Two-dose: 53.5/100k
Unvaccinated: 61.9/100k
One-dose: 30.3/100k
Three-dose: 37.1/100k
Fraser (Urban/suburban):
Two-dose: 103.1/100k
Unvaccinated: 60.3/100k
One-dose: 57.2/100k
Three-dose: 50.3/100k
Vancouver Island (Urban/Suburban/Rural Mix):
Two-dose: 53.7/100k
Unvaccinated: 35.3/100k
One-dose: 20.6/100k
Three-dose: 14.1/100k
Interior (Small Urban/Rural):
Two-dose: 53.2/100k
Unvaccinated: 40.8/100k
One-dose: 31.8/100k
Three-dose: 18.7/100k
Northern (Very Small Urban/Rural)
Two-dose: 53/100k
Unvaccinated: 26.1/100k
One-dose: 20.1/100k
Three-dose: 19.5/100k
This not only shows this pattern holding in rural areas in addition to urban areas, it breaks cases down by region type showing that within-region case rate disparity persists across the board in addition to cross-regional. The only place where unvaccinated case rate is higher than two-dose is, ironically, the most urban health authority of the bunch. Its numbers are especially suspect though as they have completely hit the wall for testing capacity. Their case numbers have been flat for a couple of weeks despite all signs of actual cases growing.
There are obviously still confounders. We don’t know the rate at which the unvaccinated seek testing compared to the vaccinated. We don’t know the degree that the unvaccinated are better at protecting themselves from infection than the unvaccinated, knowing they have higher vulnerability. No doubt there are others, but those jump out at me. However, I am pretty much convinced this is a real effect and that for the purposes of Omicron, the unvaccinated with no prior infection and the unvaccinated with prior infection are very much two different populations. As are the unvaccinated with prior infection and those vaccinated with two-doses. I think this demonstrates that refusing to accept a positive PCR test as being functionally identical to full vaccination lacks any credibility. Against Omicron it appears to be clearly superior to two doses.
Broadly speaking, third dose is appearing to outperform previous infection in this data. Though so is single dose vaccination. I have a growing suspicion that RECENT vaccination is strongly effective against Omicron. Whether it’s your first dose or your third. Recency is what 1st and 3rd doses have in common. It will be very interesting to see how third doses are holding up after 3 months against Omicron (or whatever immunity evading variant we are dealing with then.)
So far in the BC data the effectiveness of two-dose vaccination is holding up very well against hospitalization and critical care requirements. Looking at data from Alberta, effectiveness against hospitalization has fallen from about 85% pre-Omicron to about 70% as of the most recent data. Still quite a strong effect at least.
I would give the Chinese much better odds of keeping case counts under 50/million: 70%. China’s rulers are not lawyers and propagandists, agents of casuistry and illusion. They’re engineers and businessmen who have taken a mostly practical approach to the pandemic. And since learning to a large extent happens by doing, presumably their containment capability has incrementally improved. They are also willing to do what is necessary in accordance with their reality model, including firing deficient officials, as just happened again in Xi’an. The advent of Omicron means that they need to tighten travel restrictions further, which they’ve done for the upcoming Olympics. Another option is to acquire mRNA vaccines for those people who are most exposed to travel related risks. That would provide another defense line.
Xi has staked his reputation on this policy, and he’s also put the Party’s reputation on the line. This is crucial to them both domestically and for foreign consumption, to demonstrate the superiority of the Chinese system relative to America’s. Underlings who disappoint Xi are apt to face career destruction. The places that have seen massive Omicron outbreaks are also places that have let it rip. We haven’t really seen anyone try to contain it yet. Vaccination created what now seems like justifiable complacency. With the methods China has developed, I don’t think Omicron is that much more difficult to contain than previous variants. One reason I don’t give even higher odds is that Xi may discover that Omicron has something like a 0.1% mortality rate in China, which might at some point of national stress cause him to rethink the cost-benefit calculation. If a resumption of normality also occurs in the West while China suffers lockdowns, Xi might decide Zero Covid will not win the PR war. In other words, it’s easier for me to imagine them giving up than being defeated in battle.
> I’m moving towards assuming that while rapid tests are probabilistically very useful, transmission with Omicron is much faster and has outpaced the speed at which the tests turn positive, and this means that if you want to be confident rapid tests are not that useful on their own.
Can you estimate the timeline on that? If I have a negative rapid test and no human contact for 2 days beforehand, does that basically guarantee I’m not infectious?
I’d use a swab the throat not the nose, given that 2 days is pretty good, but no it’s not a basic guarantee, for that I think you unfortunately need more like 4.
If the peaks in different localities are at sufficiently different times and the peaks are sufficiently narrow, we can use America’s plan for hospital overcrowding due to natural disasters: Move people from places with overcrowded hospitals to places with spare capacity. This works great for hurricanes and earthquakes, but it hasn’t helped (much?) in the pandemic so far. The amount of time sick people stay in the hospital, or workers stay out of the hospital, is probably still going to be longer than the lag between the peaks, but it would be nice if we could use that tool again.
On your China prediction, I think that most of the remaining 60% is: China takes significant further steps in becoming more of a police state and maintains this for the foreseeable future. I’m sure whether that effects the probability of the claim or what else it implies, but it certainly will have some ramifications worth thinking about.
On the margin we should absolutely do this, but there’s going to be a lot of pushback based on ‘yes we’re not completely overwhelmed but we’re still feeling highly whelmed here and who knows what tomorrow brings’ and also this is only linear-level help so it caps out. But still worth trying.
China below 50 million: sell to 25%. My view is that most people overestimate the cost of switching to living with Omicron, e.g. “the Party has staked a lot of political capital on keeping covid out”. That’s a severe underestimate of their propaganda/opinion guidance ability. If they want to change, they will be able to do so without paying much of a price in terms of social stability.
This seems right to me. CCP can effectively disseminate whatever messaging it wants and have it appear to be accepted by populace. Couple that with how the western world will be through the brunt of this wave by late March/early April and approaching semi-normal life. The only confounding I could see is how the effective the homegrown vaccines they’ve used there are at preventing death. Although even that may not stop CCP from acting once the cat is out of the bag, which seems highly probable with community spread in Tianjin (https://www.wsj.com/articles/omicron-comes-to-china-prompting-mass-testing-and-quarantines-11641736166) and the impending influx of foreigners in Beijing for the Olympics.
Anecdata from my workplace of some dozens of mostly young, healthy employees in a high-risk setting with daily rapid tests for everyone:
-We started the Omicron wave with almost but not quite 100% vaccination, most getting 3rd doses just in the last two weeks as they became eligible
-Something like 7 cases so far this wave, most plausibly independent of each other
-Omicron outnumbers normal cold and flu cases dramatically — no one works even slightly symptomatic, and all but one person who woke up with symptoms and isolated later tested positive on RAT
-We switched to throat or combined nose+throat swabs about a week ago and they do seem to be catching cases faster, except (appropriately) in our token probably-Delta case
-… but *not one person* has tested positive without at least *some* symptoms when testing; earliest symptoms appearing a few hours up to 3 days before positive RAT (usually within 24 hours though)
-Contact tracing and isolation based on “exposure” feels rather silly now, since everyone has been exposed to friends and family all the time
-Vaccinated staff have very mild symptoms even without booster, clearing Omicron between days 4 and 7, returning to work smoothly after two negative tests
-Very small sample size, but unvaccinated staff having a rougher time and clearing virus slower
-Also very small sample size, but boosted-plus-two-weeks folks aren’t getting sick as often as two-doses-six-months-ago
-Now at a sort of equilibrium where we’re getting recoveries back slightly faster than we catch new cases
-Widespread acceptance that we’re nearly all going to get covid and it’s going to be okay
Anyway, thought that might interest some of you. Any questions, or useful experiments I could run given my smallish n? I’d love to see some more quantification with larger n by real scientists of how much infectiousness is happening in the pre-symptomatic, negative-RAT phase we can’t do anything about vs the early-throat-tickle phase we’re catching reliably. Thanks Zvi for this update, it’s very much in line with my anecdata so far!
I thought it was interesting to read here that nasal rapid tests fail to detect Omicron for several days after you become infectious, and that it appears throat/saliva tests can detect sooner. That got me wondering whether one could jury-rig an off-the-shelf rapid test to check saliva.
It turns out, a number of experts have been recommending exactly that since late December. They suggest that individuals not wait for the FDA to update on this research, and instead immediately begin swabbing their throat in addition to their nose when taking a rapid antigen test.
The Washington Post wrote an article about this yesterday: https://www.washingtonpost.com/wellness/2022/01/06/adding-throat-swab-covid-test/
I found this to be a really interesting question. So interesting that I ended up going deep down this rabbit-hole, and ultimately wrote a whole “much more than you wanted to know” blog post about it: https://brunchateleven.substack.com/p/should-you-also-swab-your-throat
TLDR: Some reputable people are recommending this, and it aligns well with recent research about Omicron multiplying faster in the throat than in the nose (unlike Delta).
If New York and DC with high vaccination rates barely manage to maintain hospital standards, I don’t know how largely unvaccinated cities will be able to fare. Maybe because their weather will save them.
Also, looking at Brazil’s case counts, they look like they’ve moved into group 1 as of today.
How can China contain Omicron with the Olympics, knowing that rapid tests no longer (usually) work for contagion? Wow what a challenge.
Military in Canada have been called to aid in flailing communities, but today announced they don’t have much capacity at the moment.
We need to be constantly reminded of what a mandated Omicron-specific booster can do to ruin most of the vaccinated’s hopes and aspirations. Read my post at the last thread.
Could China be inadvertently selecting for a test-evasive version of COVID with very long incubation times?
There’s a theory where the 1918 pandemic was exacerbated by adverse selection where the sickest soldiers in WW1 were removed from the battlefield for treatment, thus creating a selection bias where more deadly strains of the virus had a bigger chance to spread around. As a parallel, China has a hardcore quarantine regime where incoming travelers are tested every day and entire neighborhoods/cities are quarantined for massive testing. So the strain that survives has to have some of the following properties:
1. Has very long incubation times, at least in some people. 21 days or more based on Chinese quarantine rules.
2. Doesn’t cause noticeable symptoms before the virus has a chance to spread
3. Causes a larger than usual proportion of false negatives
Of course the odds of this strain evolving are pretty low given their low number of cases, but I do wonder if this is a plausible scenario.
Here in Malta daily new cases peaked on Dec 31 (with weekly new cases @ 3.6x the March 2021 peak), and hospitalizations plateaued on Jan 3, with no overloading of hospitals (60% incidentals) and with few deaths so far (perhaps 10% of the background rate). This is with about half the population boosted and with mild restrictions. So it looks to me like at least for places with a reasonable booster rollout, Omicron is not much of a problem.
Regarding the last few days of Canadian data: many places in Canada have completely exceeded their testing capacity in the last couple of weeks, and have therefore restricted PCR tests to healthcare workers and certain other critical groups in order to maintain some semblance of a reasonable turnaround time (see e.g. https://news.ontario.ca/en/backgrounder/1001387/updated-eligibility-for-pcr-testing-and-case-and-contact-management-guidance-in-ontario). Canada’s confirmed COVID numbers should be interpreted as such.
Agreed, I was going to comment the same thing. I got one of the last PCR tests available to the general public in Quebec (negative thankfully) last week. A member of the Ontario Science Table (I think) stated a few weeks ago that he thought true cases were actually 5x-8x what was being announced.
The most accurate way of judging what is happening now is hospital and ICU admissions, which are basically straight up: https://twitter.com/OntHospitalAssn/status/1479798937213091849/photo/1
Does anyone have a good sense or a reference for which provinces in Canada report hospitalizations “with” (incidental) COVID vs “for” COVID?
Apparently Ontario has not yet started distinguishing between the two, but is going to start soon. https://globalnews.ca/news/8496576/ontario-incidental-covid-hospitalizations/
Saskatchewan has started distinguishing between the two, and 40% of their COVID “hospitalizations” are incidental, and not for COVID itself. https://www.cbc.ca/news/canada/saskatchewan/saskatchewan-hopitalization-covid-19-incidental-1.6306620
I am fairly suspicious that Quebec reports incidental COVID. I have a feeling that BC and Alberta may not include incidental, but I am really not sure about these and other jurisdictions in Canada at this stage.
This distinction is incredibly important for getting a correct read on severe outcomes. I am hoping we will have national consensus very soon on reporting incidental cases separately than hospitalization for illness caused or significantly attributable to COVID. Incidental is still relevant due to infection control procedures it demands, but we need an accurate and specific picture of the relative risk of severe outcomes due directly to COVID too.
In autumn, Xi is looking to extend his term for another five years at a large party conference. Given the instability and uncertainty of what happens, if they give up on zero Covid, I can’t fathom that he would decide to give up before this important event. Afterwards, with potentially another Covid variant, and mRNA vaccines they might actually do it. However, they might just not release accurate testing numbers in that case. In fact, I don’t see why they would, it seems much more rational to just declare the pandemic to be over publicly (“we have never been at war with Covid”).
Before that, China should have enough capacity to contain the virus. Omicron has a shorter generational interval, which in some ways makes it easier to contain. Compared to Wuhan 2020, China has the capacity and the will to test everybody with PCR tests, vaccinations, and much improved digital tracking. Even if Omicron were twice more transmissible than the original strain, these improvements should offset it.
China less than 50/million (officially): 80%
China less than 50/million (actual case counts, despite being unverifiable): 33%
Buy 33% and sell 80% (e.g. I would happily bet at ~50/50 odds that China either successfully suppresses, or has to admit that it has failed).
I do think you are pointing out an important dynamic that they don’t want to admit it. But I don’t think they get much choice here. If Omicron gets substantially out, then anything short of massive obvious reactions will cause it to grow exponentially. When cases are at 60/million it’s easy to say they’re below 50. Then three days later it’s 120. Then two weeks later it’s 1000, and pretending you have containment won’t work. Trump tried this in early 2020, and found out how little time it buys.
> Generation time (serial interval) of Omicron is 3.5 days or less: 87% → 90%.
This keeps pushing R_omicron/R_delta down. I put at least 20% on R_omicron/R_delta < 1.5. By implication, at least one of {South Korea, Taiwan, New Zealand, Japan} stays below 100 cases per million through 2022, also 20%.
“Word from New Zealand in the comments is that border controls are holding for now, but that this is widely expected to fail, and if Delta wasn’t fully wiped out then I agree with this assessment. It may be a bit, but they’re going to be in group one before their winter is out.”
Delta has not been wiped out in NZ, we still get about 30-100 community cases per day. This is down from the peak of ~200 per day during the latest lockdowns which finished mid-December. It is interesting that case numbers have continued to drop without lockdowns, likely because it’s summer, and when winter comes we will get a big delta wave if omicron hasn’t hit by then.
I seem to remember the following from a discussion from about a year ago about South Africa:
South Africa is ~20% HIV positive, so there are a lot more immunocompromised people than in other countries. We expect vaccines (and maybe prior infections?) to be less effective for immunocompromised people. So South Africa will have a worse time than other places from breakthrough infections.
I haven’t seen this argument post-Omicron. What are your thoughts of how this interacts with broader questions about Omicron?
In South Africa, we would expect more breakthrough cases and higher breakthrough hospitalization / death rates than other places. Omicron’s threat outside of South Africa should be less than Omicron’s threat there.
Or maybe ~20% HIV positive actually isn’t significant enough to matter.
I definitely thought early on the South Africa was potentially a very favorable place for Omicron and it was possible the edge would be smaller elsewhere. That very much did not happen based on what we’ve seen.
This’ll be dark, but what’s your projection for China (in terms of deaths) in the 60% case where their hard containment policy fails?
Everyone poorly vaccinated at best, almost no prior cases, so relatively bad, but still much better than Delta. My median would be something like 0.2% of cases, so potentially we could see 2 million excess deaths (a lot of which would not be reported as Covid deaths).
And just like that, Omicron community transmission discovered in China.
https://www.abc.net.au/news/2022-01-09/china-mass-tests-4-million-people-tianjin-omicron/100746872
Zvi, I am very thankful for your ongoing contribution to improving our understanding and personal management of the pandemic.
1. Given the current data, is omicron ~50% as bad as delta, and are two doses of Pfizer taken 7 months ago ~80% effective in reducing the hospitalization/death risks for all groups (age/sex)?
2. I’ve calculated the infection probability with Microcovid updated for omicron, and the results are… well, weirdly optimistic?
Spending ~3 hours on my staircase during the next 8 weeks (due to taking the trash out, receiving the parcels, and going outside to take a walk), while wearing an N95 mask indoors, and having 4 infected people in close proximity (1 meter) with no masks and with an unknown vaccination status, gives just 60k microcovids (6% infection risk). This was the worst-case scenario: windows are usually open, I usually don’t meet anybody, I wear an extra visor, most people in the block should be vaccinated, and I expect less of them to be sick at any point, so the total risk decreases to… 1-2%? Am I missing something, or can I feel relieved?
1. Sounds like the right ballpark. But if you’re *this* level of paranoid I find not getting a booster pretty crazy (based on your #2).
2. Yeah, I was with the risk being low until I got to you knowing outright there was someone positive within 1 meter the whole time. Also note that risks are based on threshold effects, so *walking past* people for a cumulative hour is much less risky than one hour with a particular infected person. I do think you’re taking extreme precautions and you’re a favorite, but I wouldn’t call you a 50:1 or 100:1 favorite.
Thank you. Re: 2, I have the same 12-15 people in the entire block, and I’m almost entirely isolated from all of them unless I encounter somebody on a staircase (max. 5-sec contact). I don’t know of anyone infected, but I expect there might be up to ~4 (?) people simultaneously infected during the ucpmingpeak. Maybe my chances are ~20:1?
Yeah, I could see something like that.
> Also note that risks are based on threshold effects, so *walking past* people for a cumulative hour is much less risky than one hour with a particular infected person.
I don’t think we have any idea whether COVID infection follows a “linear no threshold” model or a “COVID hormesis” model.
But no matter the model, being within 1 meter of a person in a closed room for X minutes is probably more infectious than being for X minutes in a staircase that person was walking through – e.g. a quarantine hotel has a lot of infectious people at any given time, and very few people (I think New Zealand documented a single-digit number of cases out of >100,000 of entrants) catch COVID from other quarantinees there.
Probably a silly question: how should I handle the storage of used face masks and visors? For example, I put on an N95 mask to go outside through the corridor (for a minute or less), and then I don’t really want to dispose of it, as the mask is supposed to last for a couple of hours. I could put it in a pocket or in a paper bag, but then I risk transferring the virus from the outer layer (which, AFAIK, acts like a vacuum cleaner for pathogens) to the inside. Keeping it dangling in hand is sort of inconvenient. When I’m at home, I guess I can just carefully put it on a paper towel with the inside side, or keep it on a hanger. Ideas?
Just signal-boosting the question, more people may find the answer very helpful.
It’s not a question I think about much. I just leave mine on my desk.
> Canada is doing a more reasonable thing
Are you sure? Schools are closed again here in Ontario, for the third year in a row. My third grader has never been in a grade that wasn’t closed for ~50% of the time.
Is there any way to get information about how available Paxlovid is in different parts of the country? Seems very relevant to how Paxlovid-eligible people should be behaving right now.
Very interesting post from UW’s Institute for Health Metrics and Evaluation.
“We expect more than 50% of the US population will be infected with Omicron in the next 6 weeks.”…. “Third, a critical factor in understanding the trajectory of Omicron is the fraction of infections that are asymptomatic. Based on data from South Africa and the UK, we currently estimate this to be 80%–90%.” … ” Hospitalizations will increase to a peak that may be twice as high as last winter. These figures, however, include incidental admissions. ” https://www.healthdata.org/sites/default/files/files/102_briefing_United_States_of_America_3.pdf
12.5% of Los Angeles school kids and staff testing positive heading off of Xmas break:
https://achieve.lausd.net/covidreportcard
The IHME Model now appears to be reporting that actual Covid infections peaked back on January 6th. Is that plausible?
Source/link? Give UK did peak before that, it happening now is not impossible, but I very much do not expect it.
I’m looking in particular at the IHME graph here: https://covid19.healthdata.org/united-states-of-america?view=infections-testing&tab=trend&test=infections
That graph estimates actual infections ran about 6.23 million per day as of Jan 6, are currently running about 6.00 million per day, and will drop to about 2.2 million per day by end of January.
Thanks for delving into China, it is IMO the most interesting uncertainty at this point in the pandemic.
I don’t have anything to say to the 40% number other than I’d pick you off to the Tianjin update, moves me to 20% to put a number on it.
I think that’s too big an update purely on Tianjin, but also that’s why we don’t leave lines up all the time.
> Median peak cases day for United States: ??? → January 19, 2022
This seems about right. In southern African countries, peak cases happened on average 16 days after weekly growth peaked and 9 days after biweekly growth peaked.
In the US, weekly growth peaked on January 1, so we would expect peak cases on around January 17. Especially if biweekly growth peaked on January 8, which it seems like it did.
There are definitely wide error bars though.
Zvi, in the absence of Paxlovid, would you take fluvoxamine and/or Molnupiravir? Would your decision depend on the demographics and the severity of symptoms, and if so, how?
Fluvoxamine yes. Molnupiravir is (1) nasty enough that I wouldn’t take it unless I was relatively high risk (e.g. over 65, or somewhat younger but obese/diabetic), and (2) is a public bad even when it’s a private good because of the risk of mutation, so you shouldn’t take it if that bothers you.
OK, won’t take Molnuprivar unless there’s a life-threatening situation and there are no other treatments with comparable effectiveness. I worry about the public good, but probably would deprioritize it in this context given that I can make up for that through the positive impact at my work.
Makes sense. Remember (1) that for it to work you must start early and (2) if you start you MUST MUST MUST do the full course EXACTLY as directed, to minimize risk of creating a new strain.
Pingback: The IHME Report | Don't Worry About the Vase
>Chance we will be getting boosters modified for Omicron within 6 months of our previous booster shot: 20% (unchanged, no new info)
My question is about how you approach your models and projections.
You do have new information – another week has gone by with virtually no movement towards this prediction coming true and it is date based.
Does that mean you should update downwards slightly?
Or has your model already accounted for that?
Or is the question such that it could easily change on a dime and therefore another week passing is not relevant?
Really just curious how you think about this.
Depends what we would have expected to see within this time frame (of 3 days, not 1 week) in terms of movement towards this. We do see the boosters in development, and the decision on what to do with them is months away.
Re China: They could be stalling to see how the waves in the rest of the world play out (at the expense of some, so far limited, economic cost) to decide whether or not to let things go. The worst case scenario for them (and the rest of us) is if something more severe emerges in the course of one of these waves just as they are letting things go. I don’t really know how their vaccines compare to ours, but if China thinks they’re good enough to prevent severe disease then their actions make sense so far and their path for the rest of the year may be less bumpy than most of us expect.
Pingback: Omicron Post #14 | Don't Worry About the Vase