
I had already written most of this week’s post, and also spun out a way-too-long way-too-deep dive on what happened with a retracted FLCCC paper that that I was planning to publish today but I can’t yet because the rabbit hole is still getting deeper, when Scott Alexander posted Ivermectin: Much More Than You Wanted To Know.
My reaction to that was a deep sense of gratitude, as I was worried I’d have to write something because someone had to and no one else would. Then Scott Alexander wrote it. So now I didn’t have to. I don’t agree with every decision he made, I definitely ‘have thoughts’ and I’ll probably end up writing about that, but it can wait for another week.
There’s a variety of other stuff going on as well, including a rise in cases that is unlikely to be going away any time soon, none of it terribly surprising. Paxlovid remains illegal and somehow this may not be easy, various mandates were imposed, children noticed it was nice not to wear masks, and those against vaccination have their latest crazy nonsense where they think they can ‘detox’ and undo the vaccination shot. What a time to be alive.
Executive Summary
- Ivermectin: Much More Than You Wanted To Know.
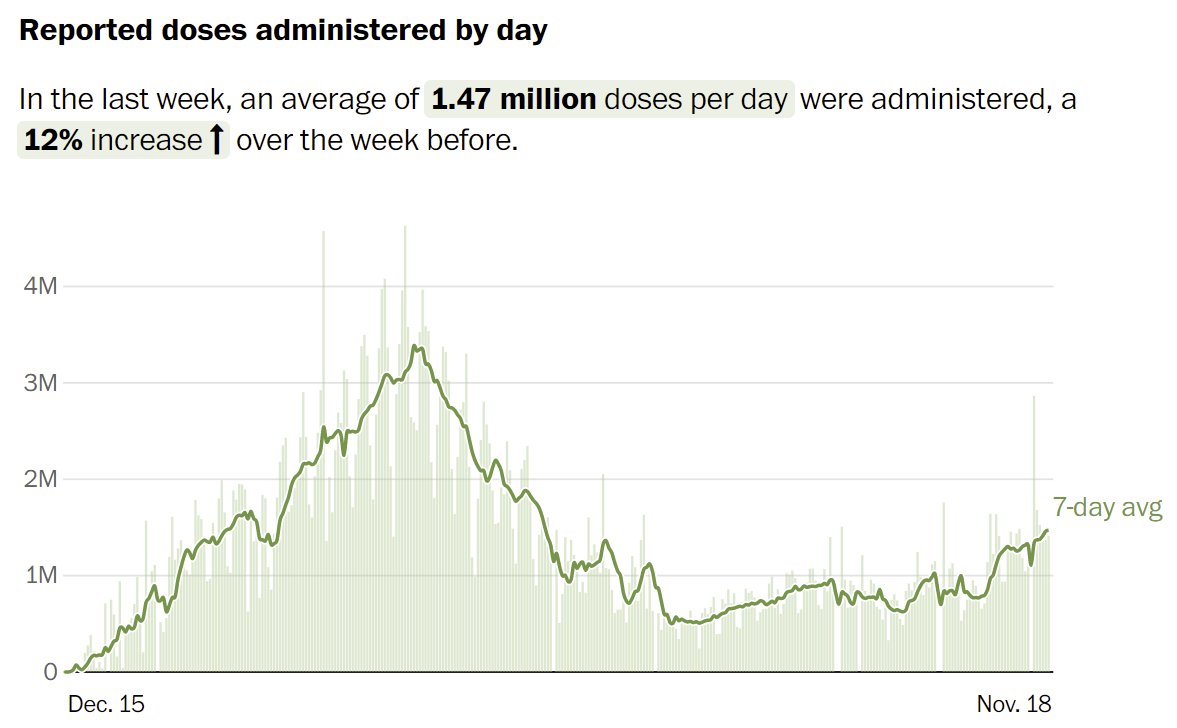
- Rise in cases is accelerating. Winter is coming.
- Paxlovid remains illegal.
Let’s run the numbers.
The Numbers
Predictions
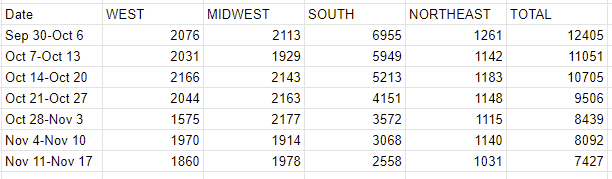
Prediction from last week (accidentally made on Monday 11/15, so it doesn’t count for prediction scoring purposes, but I didn’t get meaningful new data before then and it still attempts to represent my expectations at the time): 507k cases (+8%) and 7,690 deaths (-5%)
Results: 554k cases (+18%) and 7,427 deaths (-8%).
Prediction for next week: 654k cases (+18%) and 7,500 deaths (+1%).
Prediction for two weeks from now: We’ll see less deaths than normal due to the Thanksgiving holiday messing up reporting, and the counterfactual Zvi that didn’t put in this note likely would have forgotten to adjust for it.
Winter is coming. Boosters and child vaccinations will help a nonzero amount but they’re not sufficiently powerful to put a stop to this, and there’s very little appetite or tolerance for trying to shut things down again. There is no reason to think cases are going to stop rising any time soon, and having seen the acceleration this past week there’s a chance that the rise will be even larger in percentage terms over the next month. That means cases are likely to more than double before we peak again and it would be unsurprising if our case numbers peaked similarly to where they peaked a year ago.
Deaths
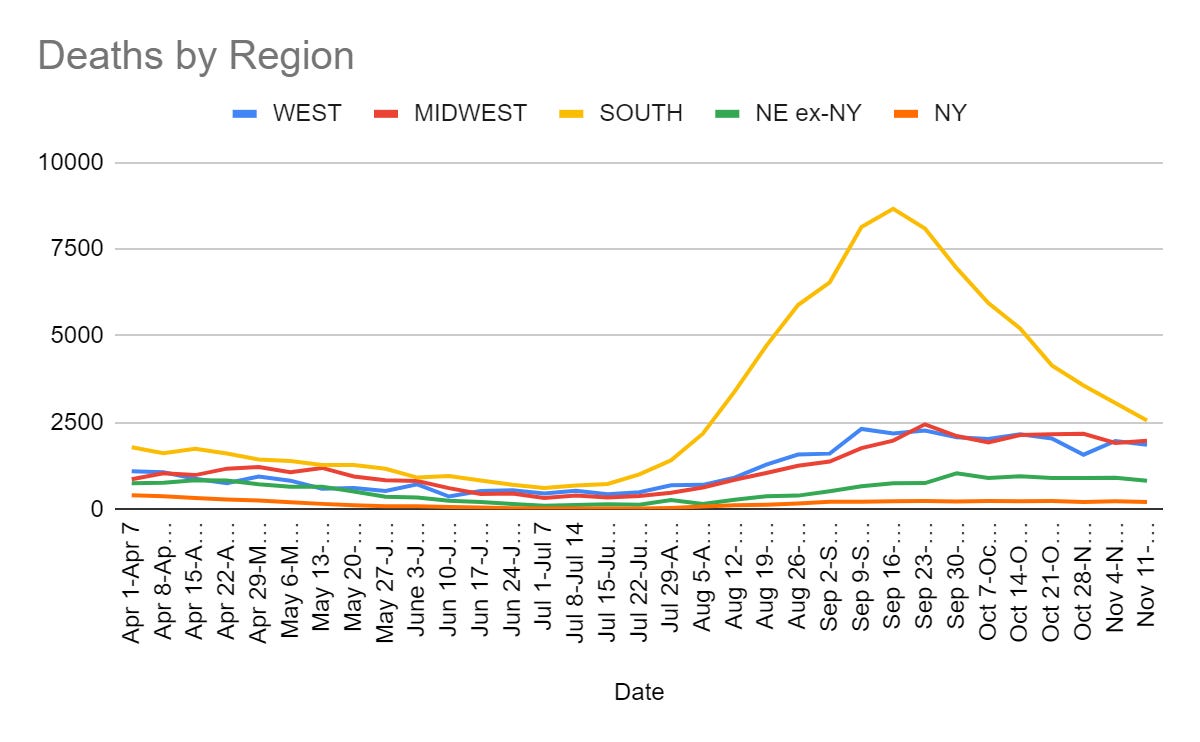
Deaths continued to decline because they lag cases. With cases rising again, this trend should reverse shortly, and death counts will begin rising again within two weeks. The only question is when, as there’s no reason to think the IFR/CFR will change much until they approve Paxlovid or (to a lesser and less certain but still probably noticeable extent) if we got more widespread use of Fluvoxamine than we currently have.
Cases
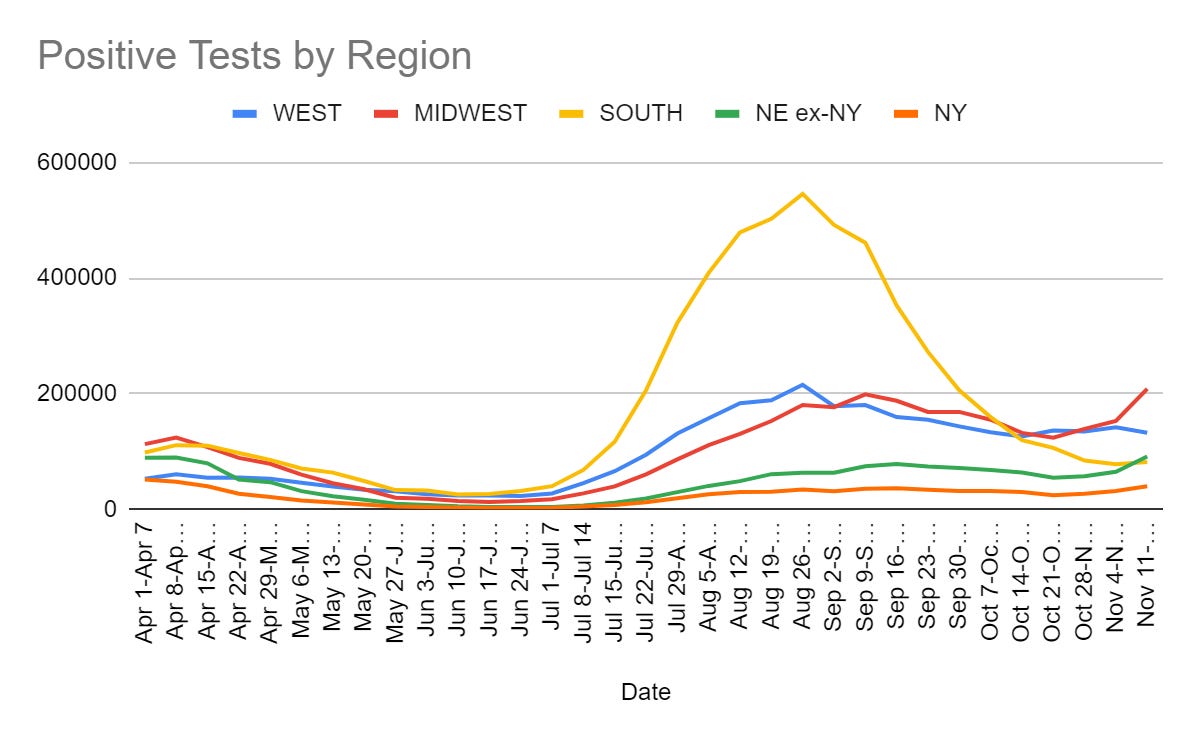
When something similar happened last year I was terrified. This year, I notice almost all of my worry is about the reaction to the coming wave. I don’t want there to be several times as much Covid-19 running around, I’m sad that more people are going to die, I’m sad about those who for medical reasons can’t get boosters, and I’m mildly worried about hospital overloads, but mostly I am worried about all the Covid-19 prevention that will result from this because almost everyone has the opportunity to get booster shots, with a booster protection is robust, and during the worst part of the wave we should have Paxlovid available, although we might still be short on supply.
It is an interesting time, in terms of intertemporal substitution. In the short term, risk is going to rise quite a bit in at least the Midwest and Northeast and probably at least the West as well, so if you have something you’d like to do a few weeks from now, it’s better to do it now while you still can and can do it safer. However, after that, Paxlovid is coming, which will make things dramatically safer again, so as long as that goes smoothly Christmas should be fine, and I’m not worried about the vacation I have planned for January.
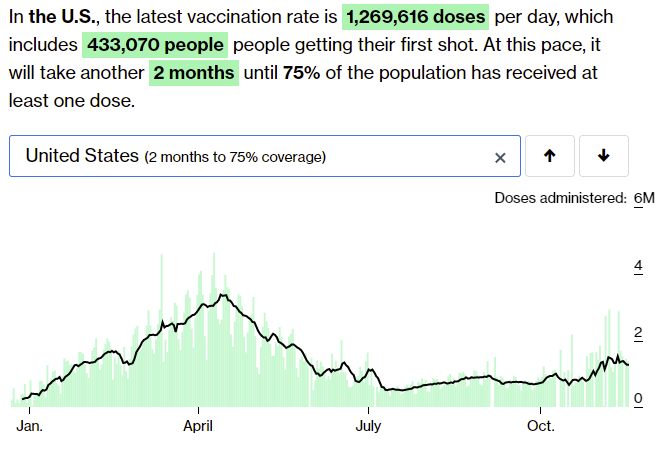
Vaccinations
The statistical implications of vaccine counts have gotten rather muddled. There’s booster shots which help but have less impact than new vaccinations, and there’s children getting vaccinated which helps but less than vaccinating adults helps. The rise we’re seeing is more difficult to put in context.

It has been two weeks since children became eligible, but it has been a very long time since parents knew this was coming, so in some ways it feels strange (even though it isn’t actually strange) that child vaccinations are moving so slowly – not that so few kids have been vaccinated so much as there are so many kids who will be vaccinated but whose parents haven’t gotten around to it yet. Some of that is logistical problems, some of that is the action becoming normal. The important question is how much low hanging fruit is available here before we exhaust the parents who actively want to protect their kids, and get into the parents that don’t want to.
This piece by Chris Arnade, called Among the Unvaccinated is a lot of where we are at. Consider reading the whole thing. The core takeaway is that being unvaccinated is core to these people’s identities, and they actively distrust both elites and all the markers of authority and credibility that the elites think give you authority and credibility, so if you’re going to convince them rather than coerce them into getting vaccinated, it’s going to have to come from people like them and it sure as hell isn’t going to be easy. Sufficiently strong coercion still does seem to mostly work.
They’re holding on to this so tightly that a new trend (as always, how widespread it actually is isn’t clear) seems to be ‘detox’ to ‘undo’ one’s vaccination. People are getting the shot because they have to, and then rushing back home to do various things that it is claimed will remove the vaccine’s effects, while often also making TikTok videos. Needless to say, this is not a physical thing one can do, and nothing they are trying does anything to interfere with the vaccine. But if one’s identity is wrapped up in not being vaccinated, it makes sense to do whatever it takes to continue to tell that story. And if you are running an anti-vaxx effort, it makes sense to be able to save face with such nonsense.
If you want details of what they’re up to, you can follow the links, nasty chemicals are involved so these are definitely not ‘free actions’ and it seemed prudent not to list it directly.
Here’s where we are more broadly:
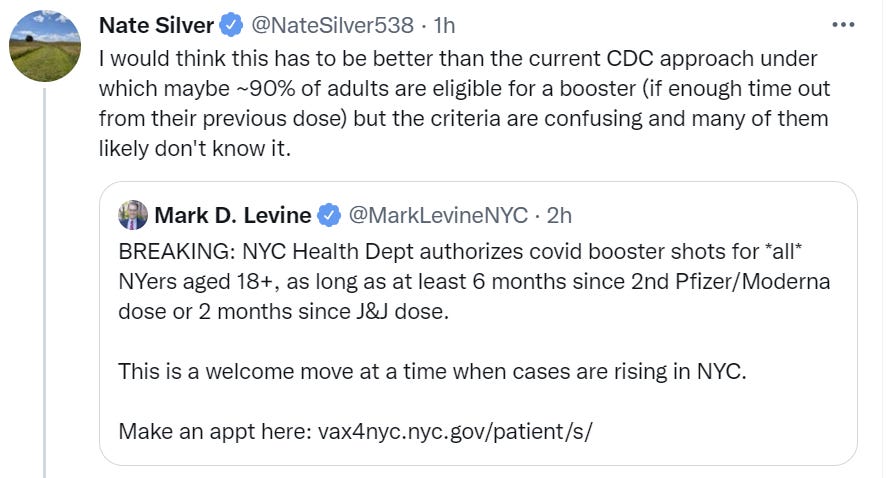
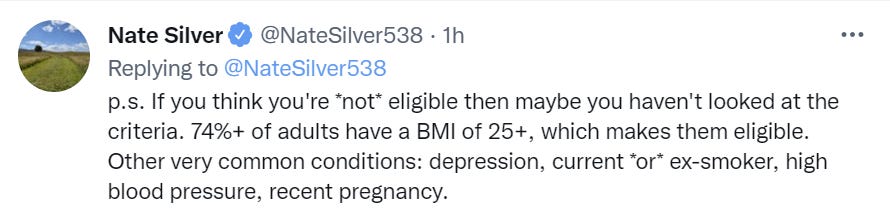
Booster shots for some, somewhat higher risk of Covid-19 and social media rants for others. Previously I’ve noted that if you wanted to be in the first category, all you had to do was check a box saying you were high risk.
The dam on even that is starting to break, and states are noticing they can they can change the eligibility rules to everyone who is 18+ years old and there isn’t anything that can stop them.
Also worth reminding people that even if you’re not in those states, and you’re not all right checking the box unless it’s technically correct, it’s probably technically correct.
Meanwhile, it’s good to persuade others to get vaccinated, and I’m not against applying a non-zero amount of pressure on them, but even when it has positive mood affiliation and makes us smile and no it isn’t a crime and the bad legal take in the other image is indeed a very bad legal take but seriously, can we please do it without committing fraud and applauding those who do? Thanks.
 of tweet by @jaheliss that attaches a screenshot of a woman in front of a computer with the text: “My roommate when she talks to unvaccinated guys and convinces them to get the vaccine so they can go on a date and then proceeds to ghost them”")
Vaccine Mandates
So I don’t fully agree with this, but I do think it’s an unusually clear and honest statement that is pointing to important things that need to be understood:
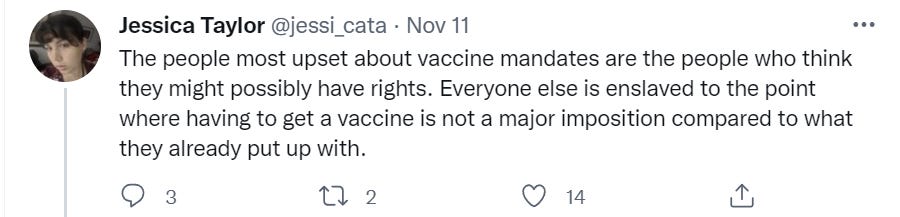
I do not think this is a major imposition compared to what we already put up with, and that is a crux for me and for many commenters from past weeks who opposed the vaccine mandate, although not one I’m looking to re-litigate. I do think I might possibly have rights, and much prefer the worlds where I have more rather than less rights, while also recognizing that there’s very little support for people having rights in the sense that I care about them having rights.
I also continue to feel strongly that if you’re going to do a mandate, it’s better to go the legitimate route and actually mandate what you want, rather than approaching the problem as if your authority is illegitimate and you have to use workarounds. And wherever you think that line is, it seems Upper Austria is well over it:

Here’s Guardian’s coverage, as well. If you’re going to tell people they need to be vaccinated in order to leave their house, it seems to me like that’s strictly worse than outright mandating vaccinations. Do, or do not.
On the plus side, if you drop by Vienna after vaccination there’s a brothel that will give you a 30 euro voucher. It sounds good at first, but that’s squarely in the range of amounts that tempt you, but where the services you’d want you can’t afford, and the services you could afford you don’t want. It’s a great publicity stunt either way and every little incentive helps, but if you weren’t already going, how often should a 30 euro discount change your mind? I also can’t help but notice that this means a bunch of still effectively unvaccinated customers are the ones newly showing up to the brothel, which doesn’t sound ideal for the workers there.
Latvia has banned unvaccinated lawmakers from voting. Given the precedent this sets, this seems like it sets the stage for much future trouble. Again, do or do not. Congressional voting from remote locations has been an ongoing strangely difficult problem this pandemic for reasons I still don’t fully understand, with congress risking outbreaks repeatedly back in 2020 rather than do what most of the country did and work remotely.
Paxlovid Remains Illegal
The great amazing news on Paxlovid is that Pfizer has signed agreements allowing others to manufacture the drug. This opens the door for much more rapid scaling up of supply, maybe even enough to treat the whole world.
Meanwhile, it remains illegal, with my explanation from last week making the rounds including at Marginal Revolution. It seems to continue to be the official position that:
- Paxlovid is safe and effective.
- Paxlovid has proven this sufficiently that it isn’t ‘ethical’ to continue running a clinical trial on it.
- Paxlovid will be approved by the FDA in December.
- Until then, Paxlovid must remain illegal.
We aren’t 100% sure Paxlovid is getting approved, but the consensus seems to be that unless there is (very unexpected) detection of outright fraud this is an open and shut case.
This seems to be a case that is sufficiently stark and obvious that a bunch of people have finally noticed the skulls and suggested maybe December should be November instead.
For example, here’s Matt Yglesias:

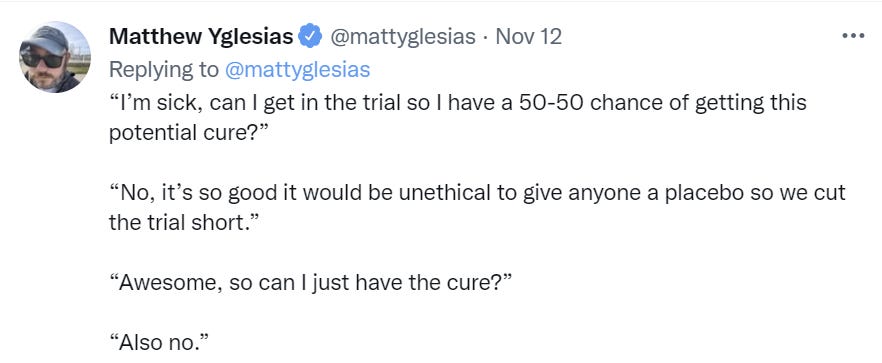
There’s the invisible graveyard caused by drugs that never got developed or approved, and then there’s the highly visible, obvious, in front of your face graveyard.
Washington Examiner points out the obvious, that the FDA is killing thousands of people by delaying Pfizer’s and Merck’s Covid treatments. It’s good to state simple things simply:
So, set Merck aside for now and consider Pfizer’s Paxlovid. In the past 30 days, more than 37,000 people died of COVID in the United States, according to the CDC . Over the next 35 days, Paxlovid could prevent tens of thousands of avoidable deaths. But instead, the FDA won’t immediately let Pfizer sell a drug it knows to be lifesaving.
This isn’t the behavior of a government set on maximizing public health. This is a bureaucracy religiously devoted to its own tedious rules to the point of defeating its own purpose for existence.
An obvious solution that is even more obviously not happening any time soon, if one cared about getting life saving medicine into the hands of patients more than other considerations, would be a prediction market for FDA approval. Thus, we could have a market on whether the FDA will approve Paxlovid within some period, let’s say 60 days, for emergency use authorization. Then, if it’s trading above let’s say 95% (p < 0.05!), we can treat that as an emergency use authorization until such time as it can be formalized.
I’ve asked Polymarket to create this market for us.
The only thing minimizing the number of lives lost, at least for now, to a lack of approval is the need to scale up supply. We don’t have enough supply to treat everyone yet, so to the extent that all doses we can create end up getting used for a while, excess people won’t die unless you count secondary effects that doubtless slowed down manufacturing.
Also, remember when I said that for all time people will question the effectiveness of Paxlovid because we didn’t run enough experiments and gather enough data? Here you go.
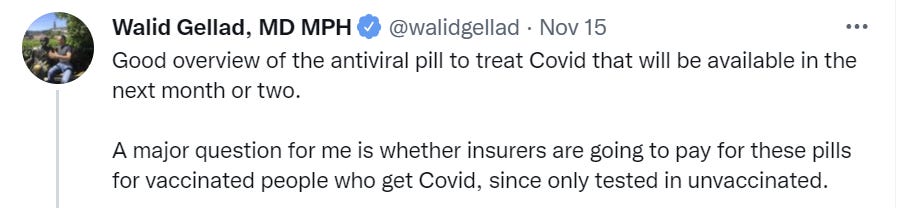
I’d be very surprised if the insurance companies actually tried to pull that stunt, and even more surprised if it did anything but blow up in their face, and when something is 90% effective you’ll know pretty fast whether or not it works.
And then there’s the article he links to, which asks the eight tough questions.
- Which pill is more effective, I mean golly, who can say.
Which one works better?
At the headline level, Pfizer’s pill reduced the risk of hospitalization and death by 89%, while Merck showed a reduction of 50%. But neither firm has disclosed detailed data from its pivotal studies, and the trials were not identically designed.
So yes, let the endless debates about the thing that we already know begin.
- Their second question is if the pills would work even better together then maybe we can use them together? And they say no, haha, of course not, that probably would work (as in save more lives) but will never be allowed.
- Will the antiviral be available for vaccinated patients with breakthrough infections?
So regulators and public health officials will have to make a judgement on the risks and benefits of the Covid pills for people with breakthrough infections — without direct data in these populations.
Pfizer is running a clinical trial, with results due next year, that does include vaccinated patients, and the company’s executives have expressed confidence based on the results so far that the treatment should work. Both Merck and Pfizer are also running studies to show that the drugs can prevent people from developing symptoms if they take the antivirals after they are exposed to the virus.
So this goes even deeper than Gellad’s concern. We might be in a position where people who have Covid-19 need to tell the hospital they’re unvaccinated in order to get treatment.
The good news is that it seems the clinical trial that includes vaccinated patients was allowed to proceed. So it’s now ‘ethical’ to continue the trial for people who don’t need the drug enough for us to be certain it works on them, but not to give it to the people who we know it definitely works on. Sounds right.
- Do the drugs work the same way? They say no, not really.
- How do they compare to monoclonal antibodies? Easier to administer, including at home, and then there’s the price. Effectiveness, it seems, is similar enough it’s not important?
- How easy will they be to get? It seems the actual question is ‘how easy will it be to get tested in time?’ which is somehow still a question.
- Will it affect a patient’s DNA? Are we seriously doing this one again? Yeah, sorry, we’re going to be doing this again.
- What will this mean for cancer patients? It seems the new drugs will interfere with many cancer treatments.
Some good information and good questions there, but it should be clear that no, absolutely not, we do not have enough information, because ‘enough information’ means ‘enough that people don’t demand more information before letting you do correct things.’ Anything less than that is not enough.
The other good news is that we can at least keep running our thought experiments, which everyone knows are better anyway.

NPIs Including Mask and Testing Mandates
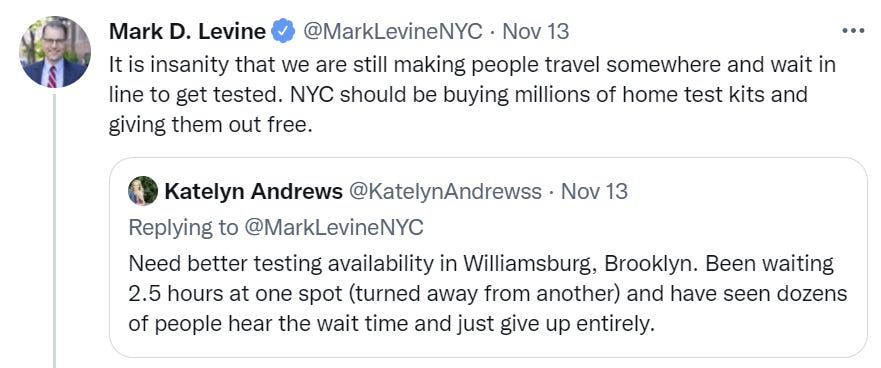
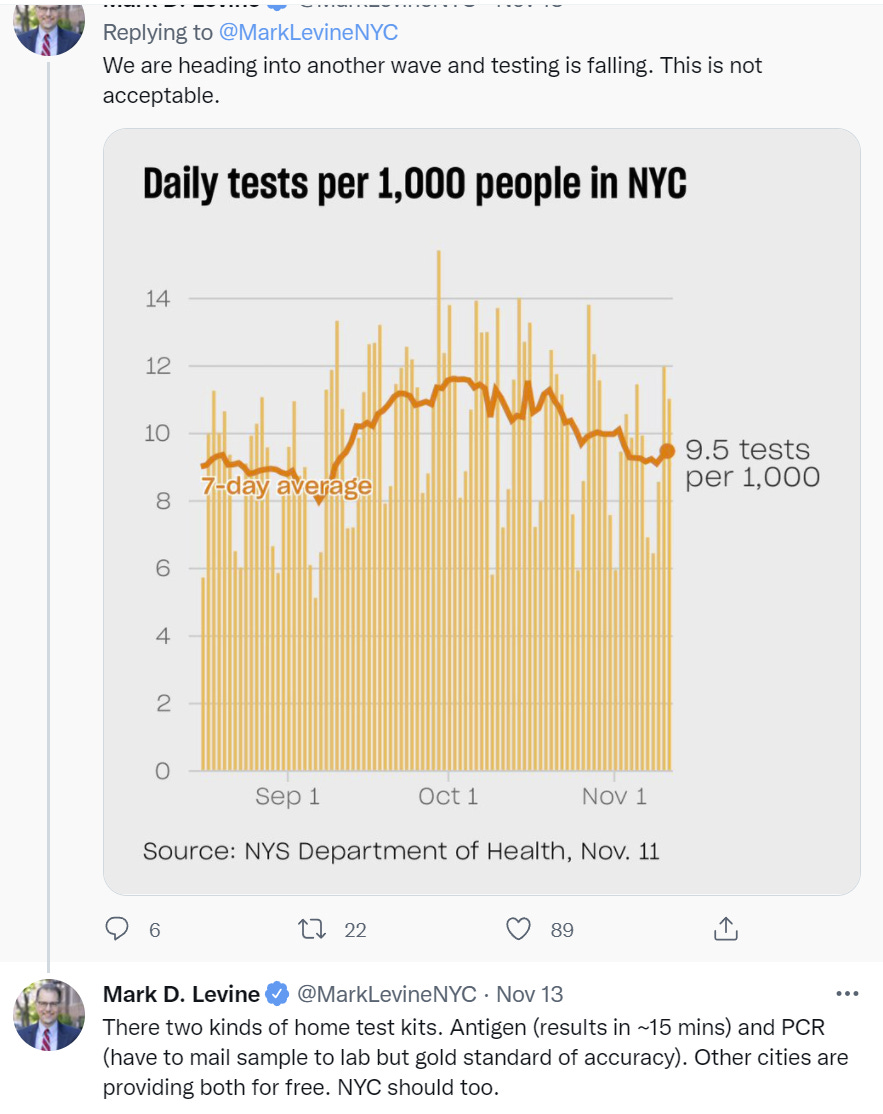
Taking an at-home test, or one where the logistics are well-handled, is cheap, and a reasonable thing to require if one requires reassurance for whatever reason.
Alas, many locales are both requiring a bunch of tests in marginal situations, and also many of those same locales are doing a rather poor job of making tests reasonably available to get. This gets rather expensive. For example here’s New York City.
On masks I’m pleased that the news seems to be about removing mandates rather than imposing new ones. Washington, DC is the latest example, lifting some of its mask requirements (WaPo).
Meanwhile, who wanted the clean glass?
I went to the bar to refill my wine glass with a second pouring of chardonnay. The bartender pulled out another, clean glass. “That’s okay,” I said, “you can refill this glass that I’ve been using.”
“No sir,” she replied. “Covid restrictions require that we always use new glasses.”
I smiled and thanked her as I took the freshly poured wine – and then said softly to myself, as I walked away from the bar needing that second glass a bit more than I did just a moment earlier, “Good thing the Covidocracy is protecting me from catching Covid from me.”
Again, the world is not right.
Think of the Children
When can vaccinated children, forced to attend schools, stop also being forced to wear masks? This NPR story asks a bunch of people that question, and gets widely varying answers. New York’s incoming mayor Eric Adams in particular says he “looks forward to it… if we can find a safe way to do it.” I believe I know a safe way to do it, and would be happy to consult with him at no charge.
Then there’s this story from WBUR, with lots of students in an ‘experiment’ allowing them to go maskless at school expressing how relieved they are to be able to hear each other properly, see each other’s faces and such. If you don’t laugh, you’ll cry. I found that story via this thread, which puts the point in stark relief.

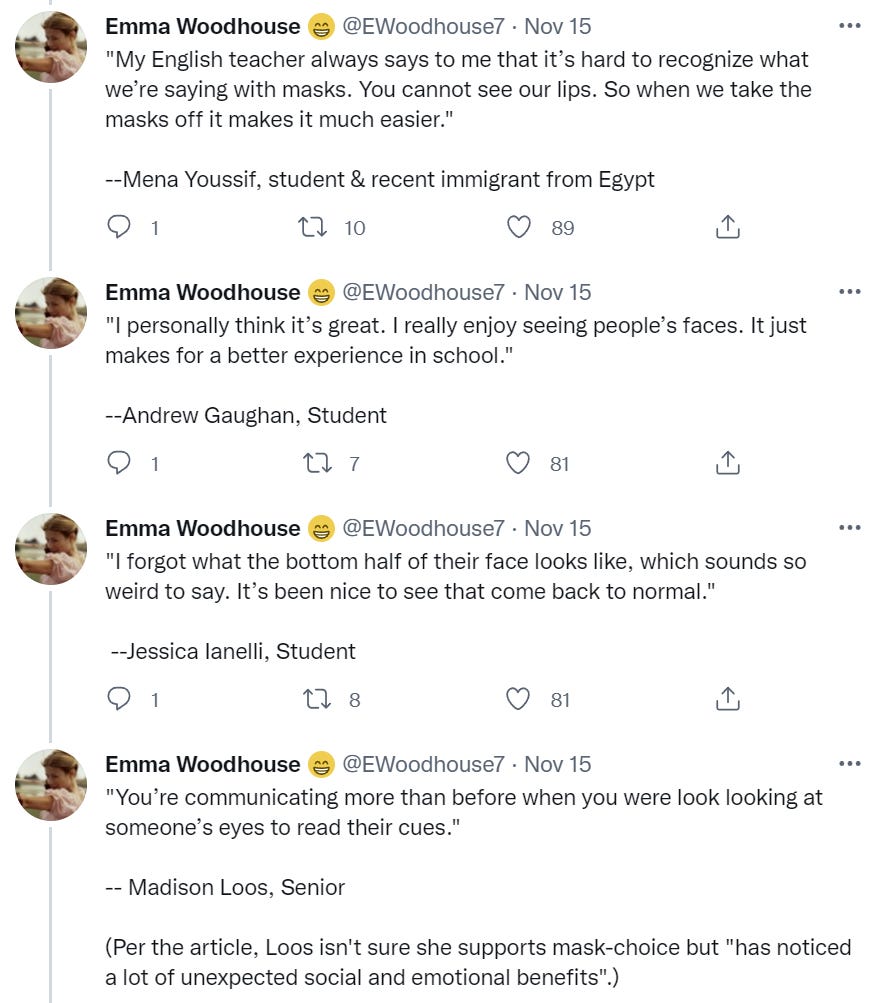

And yet the thread condemns this whole unmasking event.
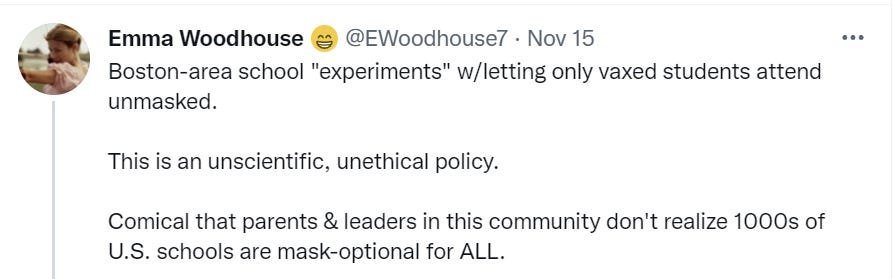
In this particular case I don’t think Emma is doing the thing where you can allow masks for all or masks for none but experimenting suddenly means what you’re doing is terrible and unethical. I think she’s merely shouting from the rooftops that it’s insane to think you need to experiment with this. I disagree, because I’ve seen time and again that there are people who don’t seem to have met their fellow human beings, and thus think that masks don’t matter, and if it takes an ‘experiment’ to show them they’re wrong, then it sure beats the alternatives.
As usual, such things also highlight how if you reversed the presumption of what is a default or what is action or what things count as risks to panic about, you see how nonsensical everyone’s actions mostly are.
Long Covid
It is always interesting when different studies live in completely different universes.
This French study claims that having self-reported symptoms associated with Long Covid is highly correlated with self-reported Covid-19 infection, but aside from lack of sense of smell, there wasn’t any association with laboratory-confirmed Covid-19 infection. Huge if true, as it would imply that Long Covid is mostly a phenomenon where people blame their long term health problems on Covid rather than a thing where Covid causes long term health problems, to the extent that they retroactively decide they likely had Covid, or perhaps also that those who think they had Covid but didn’t get confirmation often go looking for symptoms.
Then the CDC comes out and says that a full fifty percent of people get Long Covid, with symptoms that persist for at least six months. If that was actually true, we would know, because a large percentage of the population got Covid-19, so the population statistics would be screaming at us. There’s this great tidbit:
The median (IQR) proportion of COVID-19 survivors experiencing at least 1 PASC at 1 month was 54.0% (45.0%-69.0%; 13 studies); at 2-5 months, 55.0% (34.8%-65.5%; 38 studies); and at 6 or more months, 54.0% (31.0%- 67.0%; 9 studies).
So you’re telling me the percentage is the same at one month as it is at six months, and also two to five months? This has got to be some sort of fishing expedition for fishing expeditions.
My combined update from this week is to move closer to the French study’s position.
In Other News
Your periodic reminder that if we were serious about minimizing harm from Covid-19 we would be emphasizing general good health, and at a minimum we would be addressing obesity rather than pretending it’s not a thing.
The good news is that Biden finally nominated someone to head the FDA. Manchin, without whom nothing ever happens in Washington these days, responds by opposing him due to ‘ties with pharmaceutical companies.’
Some insight into the early days of the epidemic in New York, and how the state government was handling it. A good summary would be ‘not well.’ Collaborations between state and city were actively prevented.
Not Covid
Britney Spears is finally, actually free! I wish her all the best, and would like to see a gears-level evaluation of whether the Free Britney thing had an impact here, and if so how, and the dynamics involved. Like the question of the ports, this seems like a situation in which this was amplified somewhat because it presented well (e.g. it was Britney Spears and the superficial optics were terrible) and also because her whole situation was indeed objectively terrible.
Like the situation at the port, success in such an enterprise seems like it brings hope and momentum rather than causing people to be satisfied that everything is fine now. And like the situation at the port, it’s a small part of a much larger problem, in this case our rather dystopian and heavily abused legal guardian system. What we need is a way to not only free one person wrongfully imprisoned, but to change the underlying dynamics of the system.
As the thread points out, it’s also an example of earlier ‘safety’ culture gone mad, and places where rules that may or may not have made sense on a temporary basis becoming impossible to get rid of once they no longer make any sense.
Also new study suggests that psilocybin may be helpful in treating depression. I mean, yeah, could have told you that on priors, and also the results look short term enough that they don’t mean much, but hopefully these concrete particular things continue to help make various such things legal again.
Point of Order: Substack Ho?
This post was drafted using the Substack editor, as a test. My tentative conclusion is that it performed quite well aside from inability to paste from spreadsheets (I’ve emailed them to ask about that). I’ve put up a copy of the post there, so you can compare and contrast what it looks like over there. Use that comment section for any comparisons of the two versions, or to express thoughts on whether I should make the move.
Next week’s post the plan is to try out the Ghost editor.
The Lighter Side
At the movies: I was in the appropriate mood without enough time to actually go to the movies, so I saw Red Notice on Netflix. It’s living its worst life given the talents of the people involved, who make noble efforts as far as these things go. Man that was bad. No, it doesn’t make any sense on reflection. But I pretty much knew that coming in, so was it still fun? Yeah, it was still kind of fun, cause hey, why not.
At the theater: I got to see Iliza Shlesinger perform live at the Beacon Theater. She delivered the goods, exactly the way you would expect if you have seen her Netflix specials. All new material. A fine night.


Also these:



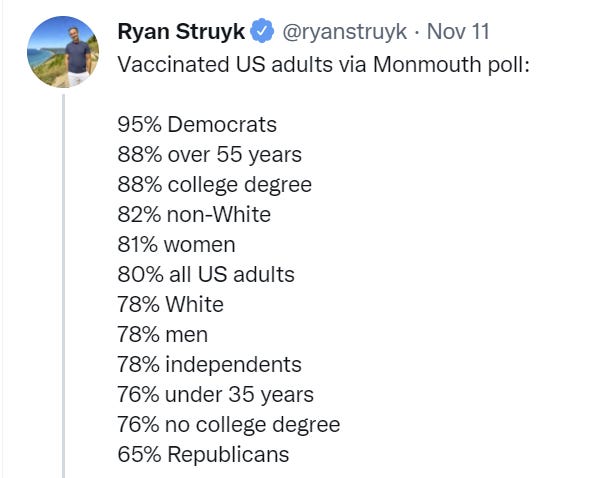
The “Monmouth poll” in that that screenshot has some questionable numbers–for one thing, their percentage of vaccinated adults is much higher than the actual percentage, based on doses administered, according to sources like the CDC.
I would be very interested to hear how they came up with these numbers, but not very inclined to trust them.
I’m guessing responding to a poll is correlated with getting vaccinated, for many reasons, and they didn’t adjust it the way you’d adjust a horse race poll. The *relative* numbers are probably relatively fine?
A lot of the statistics in here also do not line up with the “polling results”: https://www.kff.org/coronavirus-covid-19/issue-brief/latest-data-on-covid-19-vaccinations-by-race-ethnicity/
“so in some ways it feels strange (even though it isn’t actually strange) that child vaccinations are moving so slowly – not that so few kids have been vaccinated so much as there are so many kids who will be vaccinated but whose parents haven’t gotten around to it yet. Some of that is logistical problems, some of that is the action becoming normal.”
The day it became permitted by our betters for me to get my high-risk daughter vaccinated, I became a thorn in the side of every pharmacy and Dr.s office within driving distance. No one, here in the states largest metro area, had the vials of child dose available. Some of them made it very clear that if me and others like me kept pestering them they would not be able to help everyone else that came to the pharmacy for other reasons. Two said it would impossible to pull a smaller dose out of the adult vial. One said he’d lose his job if he did.
I got her vaccinated on Sunday. So, n=1, but perhaps its more about logistics.
This is rather hilarious “excuse” that they gave. Considering that giving a smaller dose requires drawing less liquid from the same vial…
The child vaccine is a different formulation (different random sugar bulk filler), diluted differently so you draw up a similar amount of liquid into the syringe. Doing smaller doses of the adult vaccine was not tested, and is not Officially Approved. Allegedly this is purely about making sure there are no issues with not drawing the dose correctly. I have my suspicions that it’s more about encouraging new sales rather than using about-to-expire adult doses, but I’m out of my depth and it could well be fully legitimate,
Can you clarify your position for me on vaccinations for kids (5-11) and masks? It seems you support both. Do you have an old posts that explains why?
I am in favor of vaccinations for children. Explanation: Personal benefits well exceed total cost, there are also positive externalities, and it enables peace of mind and helping us get less crazy with the other restrictions, privately and public too. But if you think young children are safe enough and don’t bother, it’s a small mistake.
I am for masks in the sense that masks reduce Covid-19 infection, and against mask most mandates including those in schools, but will happily honor any requests that I wear one. Explanation is that we have sufficient alternative options that are better. Note that I was strongly pro-mask prior to vaccines being available, and I would return to that position if vaccines were removed from the picture.
How much of the alarming rise in positive test results comes from selection bias as testing is increasingly focused on the unvaccinated as part of workplace mandates?
It seems to me like we need to pick between being skeptical of the usefulness of case numbers or skeptical of the vaccines. I’m in the former camp as you can probably tell.
https://coronavirus.jhu.edu/testing/individual-states tells us this is a rise in positive test percentages. Are the unvaccinated being tested more? Sure, but that makes sense, and also testing them when there’s no symptoms shouldn’t raise the positive test rate since they should still almost all be negative. It’s the tests with symptoms or contact tracing that cause high positive test %s.
It’s infuriating to me that they still don’t do some sort of random testing over time to track trends and regions. It’s such a simple and obvious thing to do, my mind goes to dark places trying to figure out what reasons they could possibly have for not doing it.
You know the reasons why, by this point, but I sympathize with your brain’s desire to pretend not to understand them.
1. If infected and with full access, would you choose Paxlovid or Molnupiravir?
2. I have a significant number of reports of long Covid from my proximate circles, and these include younger, vaccinated people with significantly pronounced symptoms. Is there a chance that it happens more often than it is usually admitted (e.g. in >10% cases)?
3. What should I make of all the news indicating a high % of vaccinated people among the Covid-19 deaths, and high numbers of cases in the highly vaccinated areas? There are many reports like these:
– https://vermontdailychronicle.com/2021/09/30/76-of-september-covid-19-deaths-are-vaxxed-breakthroughs/
– https://www.irishpost.com/news/waterford-has-irelands-second-highest-covid-19-incidence-rate-despite-fact-99-7-of-residents-are-fully-vaccinated-222363
– four weeks in the UK – 3000 deaths, 2400 fully vaccinated.
1. Paxlovid.
2. I have uncertainty but I don’t think it’s very likely.
3. Vermont has the highest vaccination rate, and that’s a total of 25 people – Vermont has a very low death rate (CFR). The Irish post is talking about infections not deaths. So that leaves the UK, which isn’t sourced. In general seems right to simply ask about the biggest possible samples and not worry about outliers – e.g. check the USA overall # and mostly use that?
I saw a poll on my local subreddit recently about how many people know someone with Long COVID: https://www.reddit.com/r/SeattleWA/comments/qu4epi/poll_do_you_know_anyone_who_has_long_covid/. 3.6% said they have Long COVID, 25% said they know someone who had Long COVID. Doesn’t seem like its particularly common, though I’m sure there’s specific circles where its more common than in others.
Confounded by age. The deaths are old vaccinated people who live in places full of old vaccinated people.
I think I have switched over the past six months from `the FDA should move faster’ to `the FDA should move slower.’ Because we don’t seem to have an intermediate setting between `forbidden’ and `mandatory.’ I expect FDA approval of Paxlovid has a substantial (est. 20%) chance of resulting in mandatory treatment with Paxlovid for anyone testing positive (with tens to hundreds of millions of people also subject to mandatory testing). If we are going to be mandating administering a pill to tens of millions, we should make pretty damn sure it doesn’t have any nasty side effects
What does mandatory administration of a pill mean? I agree it would become standard of care but that seems obviously correct? There’s always a standard of care.
Presumably something along the lines of `if you test positive you must take a course of Paxlovid on pain of (losing your job/ being sentenced to house arrest/ etc). i.e. that it will not only become the standard of care, but that refusing treatment will be prohibited by law. And perhaps, if you turn out to be allergic to Paxlovid or have some kind of adverse reaction, tough shit, you have to keep taking it anyway.
Can you give an example of a treatment via pill that causes you to lose your job or be house arrested if you don’t take it, beyond ‘stay home while you’re sick’?
Our response to covid has shredded enough precedents that I don’t find the lack of precedent for this kind of mandate at all reassuring.
The various responses are based on the need to stop the spread of infection, and to force people to do things that stop the spread. A treatment once you’re already infected isn’t in that class of thing.
It sounds like you’re basically scared that people will force arbitrary actions on you if they’re legal, and thus you’re now kind of in favor of banning as many actions as possible, or something? That the standard for a thing being legal should be if you want it to be mandatory?
I’d actually say that *even if that were true* I still think the FDA is moving too slow, but also that I don’t believe in ‘negotiating with terrorists’ in this type of way, either, if that makes sense.
“an example of a treatment via pill that causes you to lose your job or be house arrested if you don’t take it”. You’ve got the Austria story right up there. I don’t see any principled reason why ‘via pill’ is going to be the line. I can make a Devil’s advocate reason myself: if you take the pill, that shortens your viral load and infectious duration, making you less likely to spread the disease, no right to infect others, etc. Also, ‘hospitals are overwhelmed, pill reduces load’…you can follow that familiar path instead if you’d rather.
Now, I *think* my understanding of society is that adding a 90% effective treatment will cut the death numbers enough to reduce fear and hence restrictions. But I’m not 90% sure about that. I thought the vaccines would completely eliminate restrictions and that didn’t happen. So I understand Humphrey’s concern here.
Treatment for tuberculosis is mandatory and with an actual arrest and jail if you don’t
How would you suggest we “address” obesity?
I would start by suggesting that we have a norm change where I’m not instinctively terrified that I’ll be cancelled for proposing an actual answer to this question?
But to give a very clear level-1 answer, I would start by making it part of the core Covid-19 messaging that obesity puts you at high risk, that obese people need to be more cautious about Covid-19 risk because of this and that getting to a healthy weight is part of how we beat this pandemic, and other low-hanging fruit, and hope that this at least motivates a non-zero amount of self-improvement. Beyond that, it’s a good question that I need to answer *very carefully* these days so I’m not going to attempt it in a comment, but I will say that we have options.
I have a strange perspective because I used to be obese and now I’m not and I did it with diet and willpower, which is known to never work, except it did?
Don’t be afraid to hide behind an FDA Delenda Est answer here. I’ve been overweight my whole life. For my entire years, the only weight loss advice has been basically “You know you should lose weight, right” with the occasional “Do you know that you are overweight*”. I was given literally nothing actionable. I was infantilized and treated like shit by some doctors, which is common enough but more common for overweight folks.
When I really decided to do something about it, I used the tools I had in my toolbox. Fortunately, my toolbox includes an undergraduate engineering degree, a post graduate comp sci degree, and 15 years of making models. Once I learned CICO is a simplistic, wrong, but useful as most intro to thermodynamics problems, and that I could leverage my deep aesthetic appreciation for spreadsheets to the apply to this problem, I started also losing weight with diet and willpower. Obviously this solution won’t work for everyone, but I had to come up with it all on my own. And the problem was I wasn’t breaking any new scientific ground. The problem was I was the one who had to go find Rosenbaum et al (doi:10.1038/ijo.2010.184) when I stopped losing weight an instead slept for 12 hours and my temp dropped 5 degrees. My PCP with a little “Weight Loss Specialist” assertion on his door had told me that “starvation mode” wasn’t a thing. I had to learn on my own how to exercise while in a deep calorie deficit. I’ve learned more about weight management from the Stronger by Science podcast than I did from any doctor. Sorry for the rant.
Also, Wegovy is still great even if it continues to have a dumb name. I am unintentionally now doing intermitant fasting. On weekends I get up and eat as soon as I’m hungry, which is around noon or 2PM. On weekdays I eat a very solid breakfast and lunch and then usually don’t eat dinner.
*For the record, I’m about 6’5″ and according to dexa walk around with over 200 lbs of lean tissue in addition to way too much not-lean tissue. I am both big boned and fat and no one in the room with me doesn’t know that I’m overweight.
An excellent perspective, Eye Beams. Attacking obesity can be thought of as some combination of:
1. Giving people have a greater desire to have a healthy weight.
2. Giving people who have that desire better knowledge and tools.
There’s a lot of current actively backlash to and risk in doing #1, but #2 is the central thing no one knows how to solve for most people and enough progress on #2 makes #1 much less of a problem multiple ways – people get more motivated to do things they can do, that they see others succeed at, and also they need less motivation to succeed more often.
The ‘low hanging fruit’ of attacking obesity within the default paradigm would have involved some things in #2 but if you wanted to really help people, yes, you would totally blame our reluctance to allow studies and to allow people to try potential solutions.
I’d note also that in my experience, working from home (and especially fleeing to a small village) was by default bad for my health, but it also offered me a lot more control, and if I’d thought working out was the key to Covid-19 prevention, I would have been able to do that more than if I was going into an office every day…
I would expand your 2 to include those who don’t want to or need to lose weight. Not to a terribly high level, but if we can expect a 13 year old to figure out how to use a condom, we can expect them to understand CICO, progressive overload, and that a skinny person saying “Lol just stop eating when you are full what’s so hard about that” is displaying their ignornce of other people satiety signals and not their moral superiority over a glutton.
How about we require people to remain in a healthy BMI range or force companies to fire them via enforced mandates?
The explanation for the CDC Long Covid study is that they don’t bother with a control group.
For instance 30% of those surveyed have anxiety, which is probably fairly close to the general population.
I tried to access your Substack to compare the articles, but the page is marked as private so I couldn’t access it. Just letting you know in case that was unintentional.
Oh, huh. https://thezvi.substack.com/p/covid-1118-paxlovid-remains-illegal, I’ll ensure link is fixed.
This worked. Thank you.
This is the wrong thread for feedback, but after a quick skim nothing seems obviously broken. I prefer the quoted text treatment on Substack to the indented italics you use here, but otherwise I don’t prefer either one over the other.
I got to note that a prostitute in a brothel in Vienna is generally cheap, on the order of 60 euros or so, so 30 euro discount is actually huge, and places it into the “service you want but can’t afford” territory
That’s a lot cheaper than I would have expected, especially for a high quality product, and a lot cheaper than my understanding of such costs in America. Interesting. Definitely a big enough discount to matter.
As always, though, good business. Free samples!
US prostitutes are generally much more expensive than in most places, since there’s illegality premium
I’m surprised that you dismiss out of hand a possibility of dna damage by merk drug. It works by introducing huge errors in rna. Those errors are not really specific to viral rna, it affects a lot of rna’s in general. Some of the rna’s participate in damage repair pathways for dna in cells. So there’s a distinct possibility of mechanism of damaging dna in a cell, not directly, but by bad repairs (and that’s just from the top of my head). There are definitely plausible mechanisms for damage here, question is how strong of an effect, but it’s not in the realm “mrna vaccine damages dna” category, which is, indeed, total bs
Austria has now doubled down and announced both a general lockdown (that applies to both the vaccinated as well as the unvaccinated) and a duty to get vaccinated (although people will probably have until February to get the vaccine, few details have been anounced yet).
I wouldn’t regard the previous one-week-lockdown for the unvaccinated in Austria only as an indirect vaccine mandate, since it was only enacted once case numbers got really bad. Incidence rates (new cases per 100k people in the last 7 days) for the unvaccinated had been around 1200 and rising fast, while incident rates for the vaccinated and recovered were around 300. I think there is a place for a policy that says “you dont have to get vaccinated, but since you pose a higher infection risk you will have to stay at home if case numbers get to a level where icu’s capacities are threatened and we still believe case numbers will stabilize/reduce with only a partial lockdown”.
I’ll be covering next week. I agree there’s some amount of time below which it isn’t obviously worse than a full mandate, but in what worlds was this going to last 7 days and stop? I would have happily taken large bets against that when it was announced. And the moment they lifted it, they’d be right back in the same situation within a week, so…
Is there any information out there on how many people have gotten third shots?
My model is that this will be a very important determinant of outcomes going into the winter, but I am more convinced of waning immunity than ZM is.
Zvi, could you please compare the effectiveness of a “typical” treatment as of late 2020/early 2021 vs. Molnupiravir vs. Paxlovid in terms of preventing hospitalization and death?
I’m double vaccinated. If possible, should I try to get Paxlovid (and if inaccessible, Molnupiravir) for my personal use – and if needed, take it in case of early symptoms? Assume I’m a responsible person, careful with dosage, with limited access to good healthcare.
Paxlovid, as I understand it, is *on top of* any other treatments rather than being a substitute for other effective treatments, and is ~90% effective if your case is caught in time. Molunpiravir probably ~50%. You still get the old standard of care’s effects as well.
There is going to be a supply shortage so hoarding personal Paxlovid *in case you have symptoms* seems like a defection until that changes, and it’s not free in money or totally free in side effects. I’d wait for a positive test.
Regarding the “Always a clean glass policy.”
I assume the thought behind is it to prevent people from mixing used glasses, when a customer wants to refill their and some friends glasses.
Cleaning every glass is easier to implement, then making the barkeeper decide every case individualy.
Obviously one person having their own glass recleaned is kind of useless, but i remember often mixing up beer mugs when getting some for a group of friends, in pre covid times, when one would sit in crowded tents in germany, not caring about infections.
I remember such policies pre-Covid as well. I don’t think Covid had anything to do with this, and is being used to justify an existing policy.
German here. I live in this weird reality where all the media are scapegoating the unvaccinated, yet when I walked into a doctor’s office last week fully expecting to get a shot in my arm right away, they told me what they had already told me in summer: “No, you have to get on a waiting list of about 2-3 months.” Quickly looked up online if there’s anything else officially available in my city, also no. It seems to me that if you want to scapegoat the unvaccinated for all your pandemic mishandling and overreaction problems, you should at least, ya know, offer them vaccines.
This is for a first shot???
Yes. I’m not claiming there were no vaccines available during the whole year until now. Perhaps it was better in September or something. I didn’t check. I’m not worried about Covid and the only reason I checked again last week was because people keep framing current Covid restrictions as a “tyranny of the unvaccinated” (quote by Frank Ulrich Montgomery). As far as I gather, they didn’t scale up ICU capacities, and the politicians they elected keep mandating masks, threatening to close shops and so on, which is then blamed on the unvaccinated. The tone is very insulting and dehumanizing. So I felt really prosocial when I physically showed up at the doctor’s office last week. I’m sure if I spend many hours doing obscure internet research or running from doctor to doctor, I will get a vaccine in a month or two. But I don’t actually care much. Convenience matters, if I could check a box, “Bring free vaccination” while ordering pizza delivery, I would be vaccinated now. It’s not always an epic struggle between prosocial pro-vaxxers and antisocial anti-vaxxers.
I’m going to provisionally blame this on “everything in Germany is local, and some localities are broken”. If you can make it to Berlin, there are plenty of options for walk-in vaccination — I’d be happy to point you in the right direction. I’m sure the same is true in other places.
That said, I can imagine this accounting for some chunk of the unvaccinated. People try to do something once, get turned away by bureaucracy and waiting lists, and it takes a lot more effort to convince them it will be different this time.
Especially if it isn’t different the second time, which sounds like what’s happening here. The failure to even say ‘get on a train to Berlin’ when it can’t possibly be that long a trip seems pretty crazy.
I live in the South, so a trip to Berlin would be time and money intensive. I checked again online, all the bookable slots are booked out, but I did find one where you don’t need an appointment for next Saturday. Given that all the appointment-only slots everywhere are booked out, I assume you’ll have to wait in line for 3 hours or something, which technically is more inconvenient than I intend. But I’ll check it out. There do not seem to be many such options either, it’s once next week for 6 hours or so in one doctor’s office, than you have to wait at least to more weeks for the next option. At least given the information I can find online.
My hypothesis for the waiting lists and the booked-out appointments everywhere is probably bad doctor incentives plus perhaps an increase in the demand due to the fourth wave and possible political restrictions on the unvaccinated (2G rules, which means you have to be vaccinated or recovered from Covid to partake in various events etc.) So perhaps there was a recent demand surge and the options weren’t scaled up. The obvious thing to do in this case would be a quick scaling up of options.
Wow. Does anyone else have any sources beyond your personal experience? This seems insane – there’s clearly enough vaccines available for purchase that Germany can have sufficient supply, so what’s the bottleneck? Doctors not interested because bad incentives? I feel like we need to know more…
Only german sources (see below) and anecdotal experience:
1.My roommate was in the same position as Anon but got an appointment for his first dose in less then two weeks (was there last week).
2. Regarding incentives: Doctors got 20€ per admistered shot, health minister raised it last week to 28€. I don’t know if it’s financialy viable to do vaccinations for doctors. The doctors i know (family friends) are giving out vaccinations, but the majority of their work time is for “normal doctoring”. Waiting times around 1-2 months arent uncommon at regular doctors.
3. In my city, Aachen a medium sized city, there is one place where everyone can get vaccinated (1./2./3. shot) without appointment. It’s open 12:00-20:00 thought the waiting times can get quite long after regular business times. (Its in the shopping center where i buy my groceries, so i see the queues several times a week. There are 170 of these centres in Germany.
4. Also there are “vaccination busses”, mobile opportunities to get vaccinated without appointment in Aachen and surrounding cities. Around 700 of these are driving around germany.
Links:
Doctors payment, number of centres and busses/mobile teams
https://www.aerztezeitung.de/Politik/Spahn-Aerzte-sollen-hoehere-Verguetung-fuer-Corona-Impfung-erhalten-424387.html
A site dor Germans to find vaccination opportunitys in their area:
https://www.zusammengegencorona.de/impfen/#deutschlandkarte
Yeah, I’m not going to stand in a queue for 3 hours. After being insulted as a “tyrant” for not getting vaccinated, that’s an unacceptable demand to make by those who, unlike me, actually care about Covid. The arguments were sound in March 2020 when we didn’t know how deadly this is and needed time to scale up the ICU. Now I just don’t care. Scumbags like Frank Ulrich Montgomery have lobbied against our rights and liberties for years before this pandemic; it’s unsurprising to hear such insults from him while there is no convenient vaccination effort. I think it’s fitting that the World Medical Association chose him to represent them; I think they chose him *because* he’s a disrespectful authoritarian scumbag and it accurately reflects their arrogance and terminal values. After these insults, the correct expectation to have on my end is not, “Spend several hours doing online research and discussion and then physically stand in line for 3 hours so I can fulfill the insulters’ demands”, it’s “Bring the vaccine to my home at the time of my leisure and leave a free pizza too boot”.
“Washington Examiner points out the obvious, that the FDA is killing thousands of people by delaying Pfizer’s and Merck’s Covid treatments.”
So, situation normal, all f’d up?
It all depends on your baseline. From mine/ours, the Examiner’s report indicates more willingness to call things what they are, which is good news.
Some doubts about the French long Covid study:
https://www.methodsman.com/blog/is-long-covid-real
As far as I can tell, the study doesn’t adequately account for the decline of antibodies over time. Therefore it’s unclear that the stated 87% sensitivity of the serology test holds. But, their failure even to mention the major issue presented by false positives in their study invalidates their conclusion.
The other long Covid study also looks like garbage. The average patient was 54 years old–which is not the average age of infectees–unrepresentative. They’re also only picking up those with known infections, who disproportionately have serious infections.
On the French study, if we were looking for a small effect I would agree that such concerns invalidate, but because the claimed effects are large I’m not sure and we need to think more? As in, if there’s almost no correlation between test and symptoms at all, what does that imply about the error rate if the symptoms are caused by the thing? Suppose the test was right 80% of the time and wrong 20% of the time in both directions. You’d expect to see 60% of the ‘real’ correlation showing up.
(Note that I’ve thought about this concern for like 1 minute and didn’t look carefully)
The other study is doing the opposite, you have to cut it down some the other way, but still seems like If True then you say this thing about that subgroup and still conclude something meaningful?
Let’s take their numbers at face value to begin with, including the accuracy of the serological test. In doing so we find that 2 of the 4 quadrants into which they divide their subjects are highly unreliable and 1 is of dubious reliability. They claim the test has 87% sensitivity and 97.5% specificity.
That sensitivity would lead to 140 false negatives, to be distributed in the first two quadrants. The first quadrant–people who tested negative and believe themselves negative–is highly reliable and contains 25,271 people: only 140 people could be misclassified in this group, 0.5%. Quadrant 2 (negative test, positive belief) has 461, of whom 140 could be misclassified, a possible error rate of 30%.
The specificity rate equals 644 false positives, distributed in the second two quadrants. Quadrant 3 (positive test, negative belief) has 638 people, with a possible error rate of 100%. Quadrant 4 (positive test, positive belief), with 453 people, could also have a 100% error rate. Of the 1,091 people in these quadrants, 644 are false positives: 59%. And they state that 4% of the study population ought to have been infected based on the rate of infection in France at the time, yet according to these numbers we derive a total of 447 + 140 = 587 infections, 2.2% of the study population.
That’s the face value of the numbers they present. I think these inconsistencies and misclassifications overwhelm the study. But, that’s just the surface trouble. Then, we have to question whether the accuracy of their test is what they claim. I suspect more false negatives than their number claims–due to antibodies waning over time–and I suspect these people are concentrated in quadrant 2. This would explain why they found 2.2% true infections rather than 4%. I would not be surprised if over half of quadrant 2 are false negatives. Then we have to wonder how many of the 1.7% in quadrant 2 have fallen into psychosomatic illness in the current media/cultural environment. Quadrant 3 is probably loaded with false positives, well over 59% if their specificity number is right.
In short, I think quadrants 2 and 3 are highly inaccurate and of no use for comparison. GIGO. But, if we only compare quadrants 1 and 4, the study offers nothing new.
We need a trolly problem meme where taking no action saves lives but only half of the time, and flipping the switch kills everybody all the time, but the FDA is operating the switch.
What is the risk of contracting Covid-19 from surfaces (e.g. unwashed groceries, door knobs previously touched by hands touching unclean things)? I know it’s very low, but I’m curious about the general range.
Also, why aren’t there any booster shots specifically based on the delta variant’s mRNA?
Second this. What if the risk of getting Covid-19 from disinfected groceries is just 0.001% each time, but you have hundreds of such situations happening to you and your flatmates, so it gives a 10-20% total risk of infection over the course of a couple of months?
Re: vaccine, maybe it’s the inefficient system of manufacturing (or approving) vaccines. Or maybe it’s against the financial incentives.
*non-disinfected, typo.
My answer is something like:
1. We don’t know the actual answer because experiments are illegal, so I can’t say e.g. 10^-9 or whatever, plus there are various variables.
2. In order for a surface to infect you it requires you to touch the surface then touch your nose/mouth/eyes or at least face before you wash your hands sufficiently, so you can reduce this risk to epsilon if you care enough.
3. In practice, even if you ignored surfaces as a risk factor, provided you weren’t being super ultra otherwise paranoid, I’m confident your risk would not noticeably increase.
The booster shots weren’t modified because the thing they target didn’t change, I think, or at least not enough to matter, or not enough to justify the extra regulatory issues involved.
Michael Mina has been pushing this concern about the un-reformulated vaccines. I believe that at least some of the variations in the Delta variant are in fact in the spike protein. He makes the also excellent point that since nearly 100% of all cases are now the Delta variant, any *new* variant is almost certain to incorporate the changes of Delta and just have additional ones, so we might as well have a vaccine that teaches our body to recognize the Delta specific spike rather than the slightly different classic spike.
I get the impression it’s mostly about the changes being relatively small, and the difficulty of getting the change approved is high enough that it’s not worth pausing their factories for the time needed to start manufacturing the new one for the tests, and then switch them all.
Pingback: When Will The FDA Approve Paxlovid? – Actuarial News
How does fluvoxamine compare to Paxlovid in terms of effectiveness?
My best guess is Fluvoxamine is mean ~25% effective and Paxlovid is ~90% effective.
I also don’t know any reason you can’t use both and get to 92%, but am of course less confident there.
On thought experiments, this satire piece from a decade ago was very amusing to analytic philosophers – not sure if it’s as amusing to people who aren’t as familiar with Kripke, Putnam, and Williamson.
Pingback: Covid 11/25: Another Thanksgiving | Don't Worry About the Vase