
The pandemic has become predictable, which is the world we much prefer to live in. Cases and deaths continue their slow but steady declines, vaccine approvals for boosters and children continue to slowly move forward. Mandates continue to make people angry but mostly work when used, while also not that often being used. Same old, same old.
The big news story was that one of the studies of Long Covid was revealed to be vastly overestimating frequency due to a methodological ‘error.’ It’s an important update.
Executive Summary
- Cases and deaths declining as expected.
- Approvals progressing slowly as expected.
- Long Covid study had important error, see discussion later in post.
Let’s run the numbers.
The Numbers
Predictions
Prediction from last week: 560k cases (-10%) and 11,500 deaths (-8%).
Results: 547k cases (-12%) and 11,051 deaths (-12%).
Prediction for next week: 481k cases (-12%) and 9,835 deaths (-11%).
We are still in a low-variance situation, with no reason to expect any big surprises for at least several more weeks.
Deaths
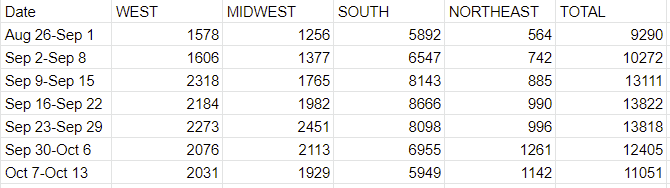
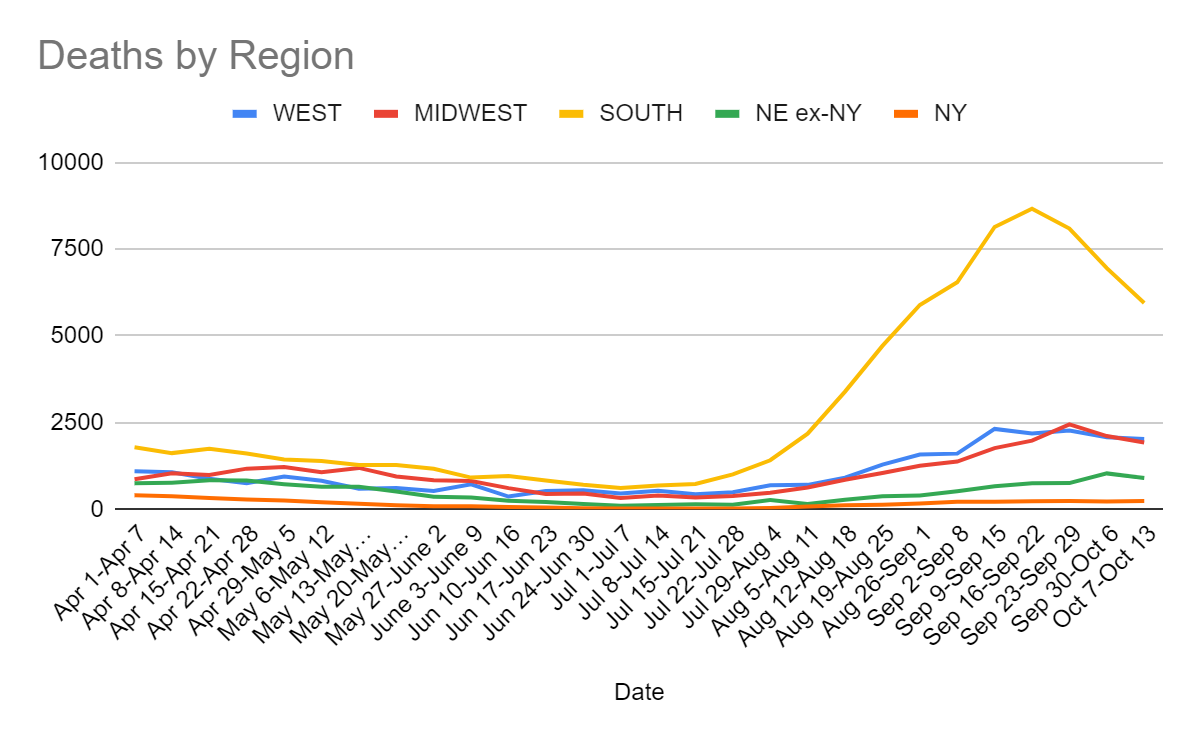
The exact rate of decline here was a pleasant surprise, but we’ve gotten to the point where this is a lagging indicator, so the times when it is surprising are mostly about data gathering issues, either holidays or changes in the ways in which we do testing. Expect this trend to continue, and continue to mirror cases with a lag.
Cases
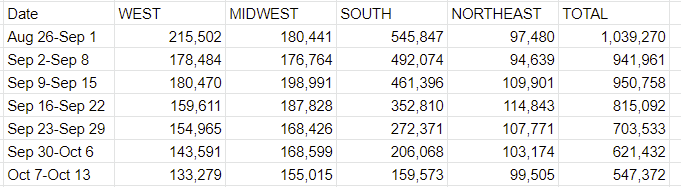
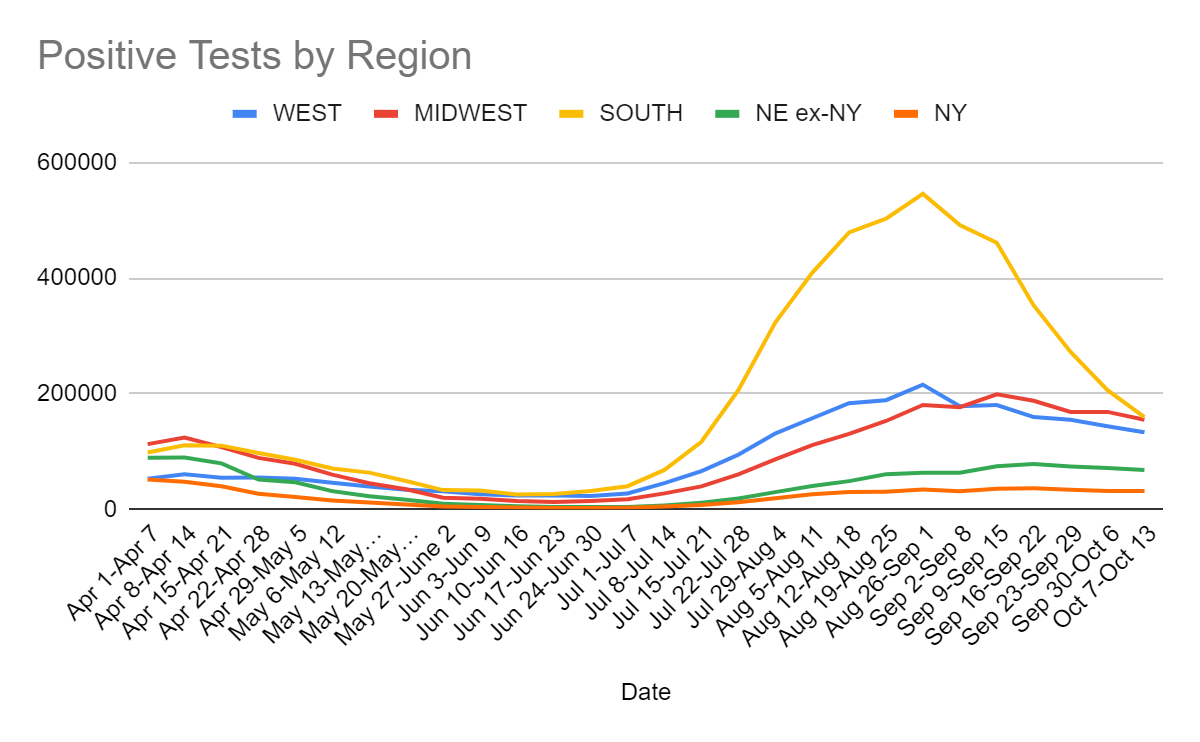
This is pretty much exactly what we would have expected. The Northeast number is slightly disappointing, others were slightly better than expected, but no real surprises.
Vaccinations
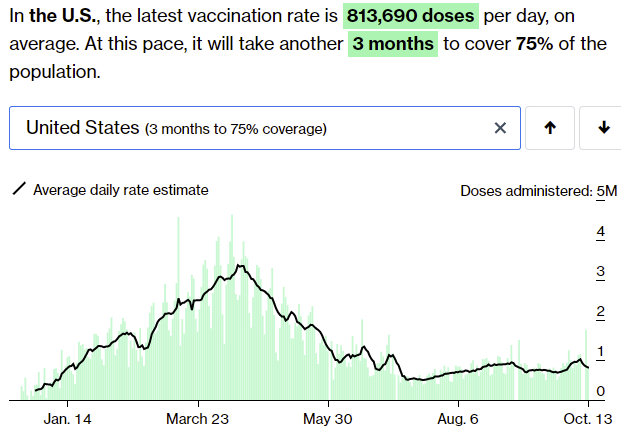
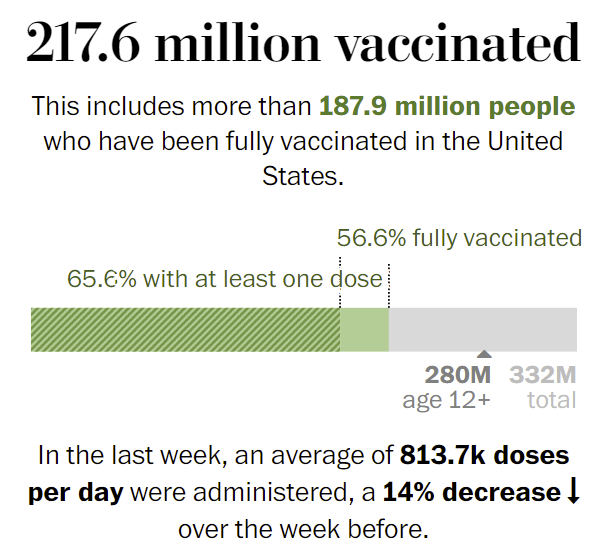
The rate of vaccinations continues to not change much, and it’s clear that the positive bump wasn’t the start of a surge. That continues not to tell us much about how much work the mandates are doing here. My impression is that the mandates that have teeth work, but that few of them have teeth.
In his podcast interview this week with FiveThirtyEight, former FDA Commissioner Dr. Scott Gottlieb asks where the cost-benefit analyses are on the vaccine mandates, since there don’t seem to be any. He estimates that we could use mandates to go from something like 80% adult vaccination rates to 84%, and asks how much that really accomplishes.
My answer is that this change would be worth quite a lot, but how much depends heavily on how we would react to the two scenarios.
Cutting the number of unvaccinated adults by 20% wouldn’t cut transmission by 20%, since there is some spread by non-adults and some spread by the vaccinated. It’s still a major percent drop in transmission if behavior didn’t adjust, at least 10%. Cutting transmission by 10% means a 10% cut in cases every four days or so if behavior doesn’t adjust, which is a rather big game, cutting cases in half each month.
Behaviors would of course adjust, which is a big benefit. We’d get to increase our equilibrium amount of Covid-19 risk by 10%, which is a substantial percentage of the way back to regular life. If we used this to eliminate ‘stupid prevention’ selectively the win would be even bigger.
Alternatively, if we didn’t adjust our behaviors, then we get full suppression before too long, or damn close to it, at which point the adjustments happen no matter what any ‘public health experts’ or government officials might want. If we’re looking at under 10k cases per day, as we likely are within a few months, people outside of some particular institutions going to go back to normal, and even in those few places there’d be increasing pressure over time.
The intuition pump here is that putting us over the top is a huge deal, and that this is plausibly exactly what we need to get over the top, and if this doesn’t get us there it still gives us a bunch of extra slack to spend. Plus it creates new ‘safe spaces’ where everyone is vaccinated. And of course, it lowers average severity that much more, as well.
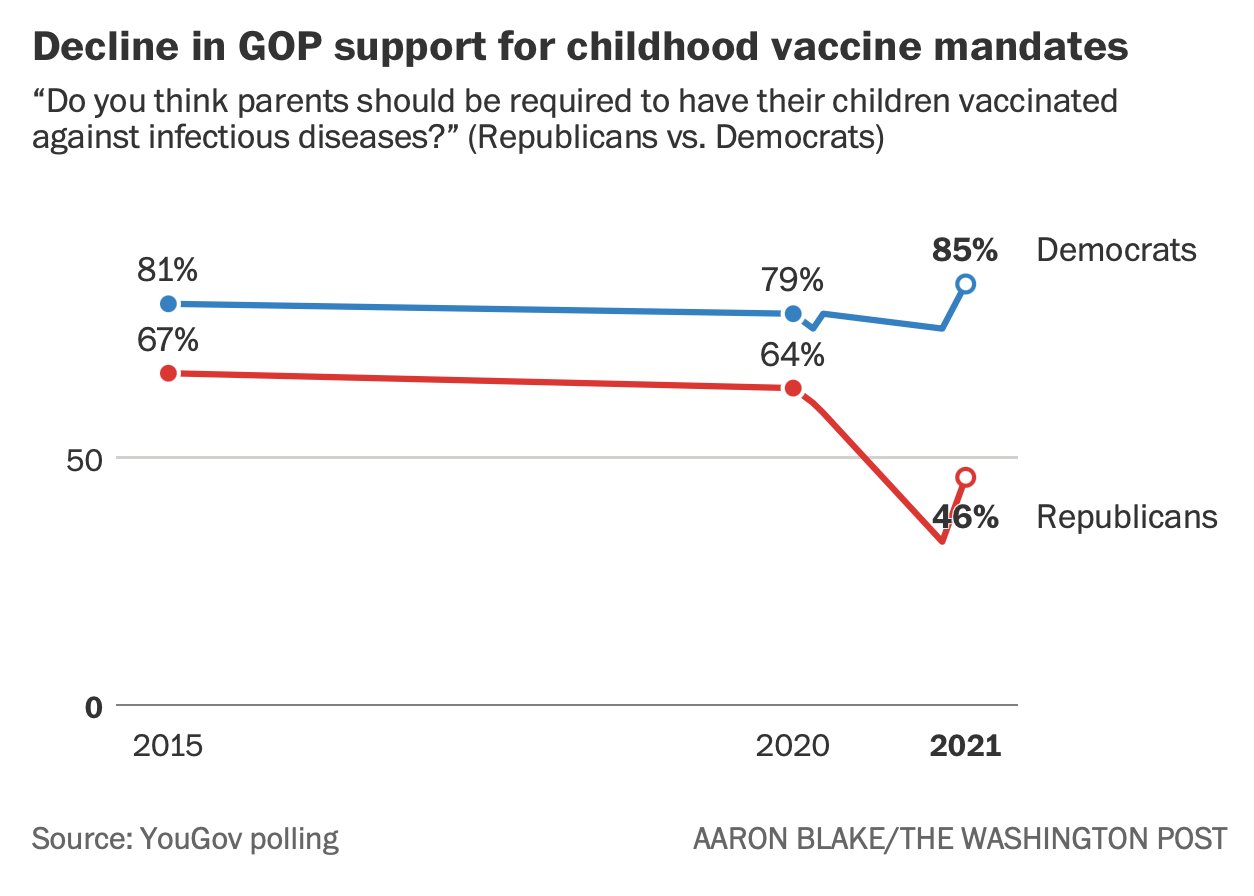
One big cost of all this is that Republicans are turning against vaccinations and vaccine mandates in general, which is a big problem, but the timing seems to correspond to the vaccine rollout rather than to the mandates. Not clear to what extent the mandates will contribute to this, but would be rather disastrous if red states stopped requiring childhood immunizations.
Looks like mix and matching vaccines is going to be shown once again to be effective, but this time the results come from America, so maybe they will count.
Vaccine Mandates
The mandate conflict this week is that Texas mandated a lack of vaccine mandates by any entity at all, to combat Biden’s mandate that there be mandates for large corporations, putting the two in direct conflict. There’s still a technical way out of that for corporations, which is that the Biden rule allows frequent testing as an alternative. Alternatively, one can take a side and say that the Texas rule is invalid, which is what the Biden administration is claiming, and the major airlines seem to have adopted this policy.
Mostly we didn’t hear about much in the way of new mandates this week. The mandates that are already in place or being put in place seem to be proceeding smoothly, but there isn’t much appetite to add new ones.
Meanwhile, given the lack of enthusiasm for surprise, ruthless efficiency or fanatical devotion to the Pope, some vaccine advertisements turn to fear.
In other places, some countries are actively halting or scaling back use of Moderna, despite it being clearly the most effective vaccine, due to relatively trivial concerns. I can’t even get angry about it anymore, but all the more reason to get your shots while you can to be safe on multiple fronts.
The FDA is moving forward with child vaccine approval (after which it will presumably become mandatory right away in many places) but isn’t comfortable yet that it has inserted enough delays to make everyone feel comfortable, so the delays continue for now.
Long Covid
Via an excellent comment, we have an important discovery about the Long Covid data.
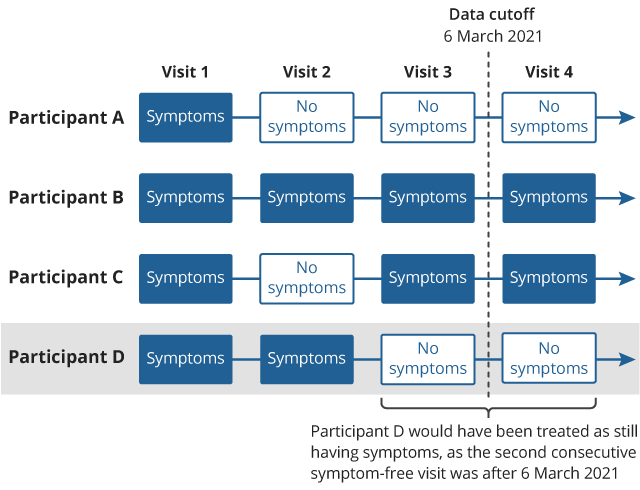
A major source for the previous pessimistic LC estimates, like Scott Alexanders (the UK’s giant ONS survey) published an update of their previous report which looked at a follow-up over a longer time period. Basically they only counted an end to long Covid if there were two consecutive reports of no symptoms, and lots of their respondents had only one report of no symptoms before the study ended, not two, so got counted as persistent cases. When they went back and updated their numbers, the overall results were substantially lower. This graphic explains their original mistake:
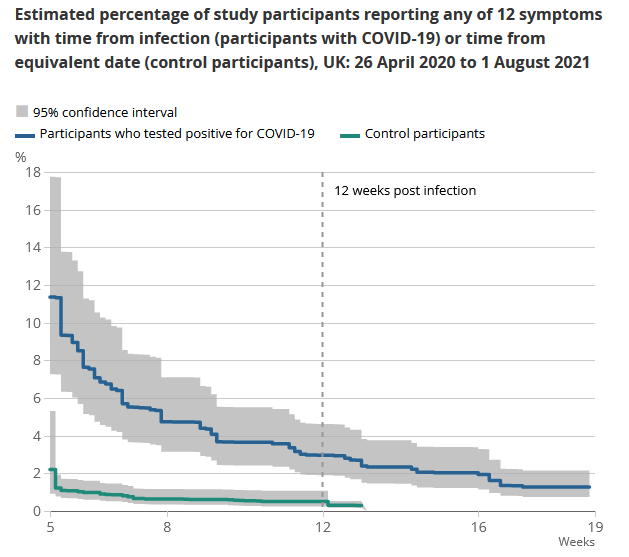
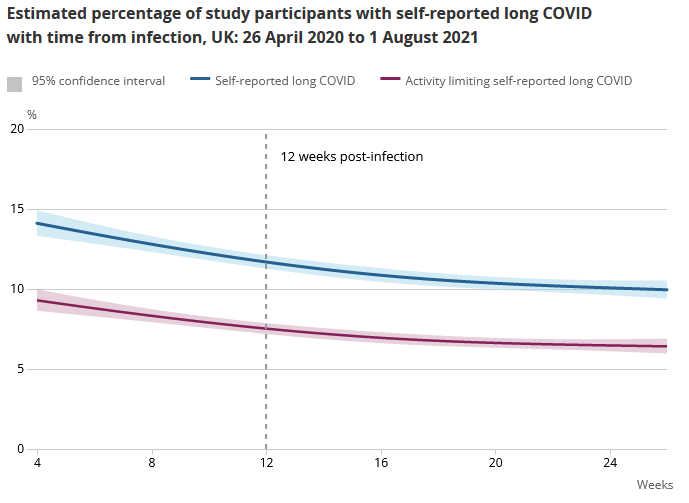
The new headline result is 7.5% of Covid-19 patients had ‘some limitation’ of daily activities after 12 weeks if you ask them if they had long Covid-19. If you go by asking if there were any symptoms from a given list, the rate is lower (like 3%). The full reportis here. What’s notable is that a lot of participants reported LC symptoms with no Covid-19 positive test.
They break it down by age and sex in the full report, but you should treat these numbers as numbers for mostly double vaxxed AZ and some mixture of single/double vaxxed Pfizer/Moderna for younger groups, since that’s how it worked in the UK.
This is a pretty dumb error, a very dumb way to get a lot of people very scared and destroy a lot of value. Many thanks to the team for correcting the error, whether or not it was intentional and whether or not they should never have made the mistake. And whether or not the mistake was a reasonable one to be making, which it pretty much wasn’t. Error correction is a big deal. Basically what they did, as far as I can tell, was this:
- If you report symptoms, that means for now you have Long Covid.
- If you report no symptoms twice in a row, congratulations, you don’t have long Covid.
- If you report no symptoms then symptoms, we still assume the symptoms are due to Covid, and you therefore still have Long Covid.
- If your last report was no symptoms, you’re still considered to have Long Covid until you report in again with no symptoms.
- A lot of people didn’t feel the second no-symptom report was a terribly urgent thing to be doing.
- A lot of people simply hadn’t had the chance to report a second time once their symptoms had cleared up.
- Yet they still counted the period that included their report of no symptoms, as a length of time that they had Long Covid.
To be blunt, they cheated (intentionally or otherwise), it was a massive effect, and we should have caught it, but to my knowledge none of us did. They have now fessed up.
If you ask people to pick from a list of common symptoms, only 3% report that they have one. The larger numbers are mostly or entirely what happens when people are asked if there is anything wrong with them at all, and would they like to blame it on Covid-19. Also the percentages declined a lot over time, so chances are few of the cases would be permanent or semi-permanent. Even if you buy one of the larger numbers, this is a substantial improvement.
Given how many people have already had Covid if you go by the antibodies present in various populations or what I would otherwise guess, this seems far more plausible, that Long Covid while real is relatively rare.
NPIs Including Mask and Testing Mandates
The other thing I wanted to highlight from Gottlieb’s podcast interview this week with FiveThirtyEight was that when cloth masks were first proposed as a solution, everyone involved (according to his account) agreed that cloth masks probably worked, and agreed they were widely available, but that they pushed back hard because if people were told they could use masks, they wouldn’t listen to demands that they stay inside. So that’s the type of thinking we are dealing with there. Scott Gottlieb is very much in the ‘level with the people and it will work out’ camp, and I continue to wonder about the alternative world where he had still been in charge at FDA in 2020.
Lateral Flow Tests looking more effective in practice than we previously thought.
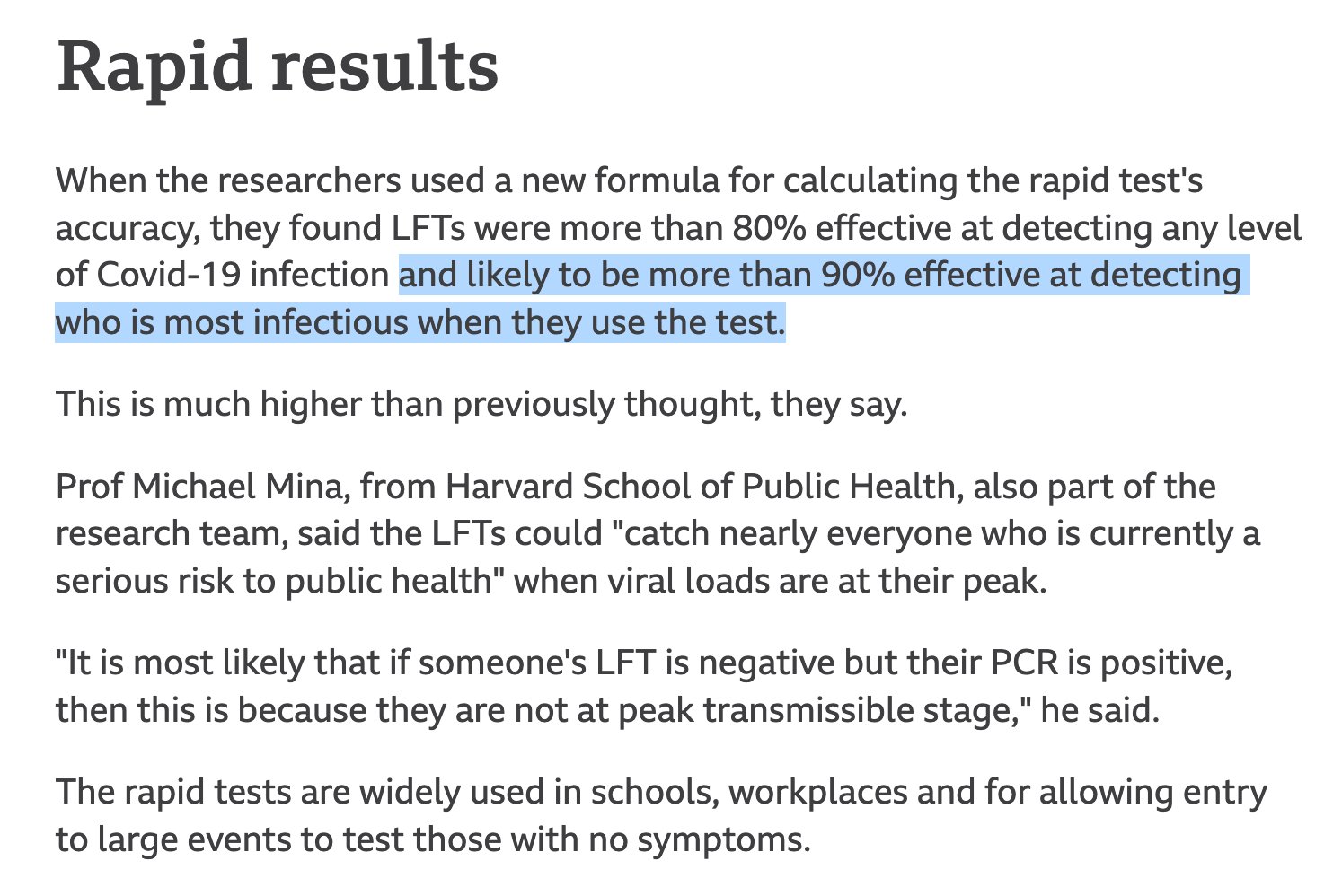
Good thing we blocked them due to being insufficiently good, leaving many people without any access to testing when it mattered most.
In Other News
There were a bunch of flights cancelled in Florida, over some combination of a lack of pilots due to protests against vaccine mandates, a lack of air traffic controllers due to protests over vaccine mandates, and bad weather, depending on who you believe. In the mainstream media this has been treated with something that’s hard not to describe as a media blackout, where a big event happened with both practical short-term and potential long-term impact, and everyone somehow decided not to cover it. It seemed to reflect prioritizing something other than reporting newsworthy events or providing useful information to listeners and readers.
On the other side, this was seen as some glorious sign of revolt and things to come, which also seems mostly wrong to me. Such disruptions seem both rare and mostly not that impactful, with this being news exactly because it had any meaningful impact at all. Whereas supply chain issues caused by actual Covid-19 disruptions are increasingly dire.
Ivermectin studies looking more and more like outright fraud, as in the study never happened and they copied lines of data a lot levels of fraud.
Another reminder of how bad it’s been that we’ve groundlessly scared pregnant women to the point where they’re largely not getting vaccinated, and now they’re filling ICUs.
Dr. Sanjay Gupta appeared on the Joe Rogan Experience. Due to time limitations I haven’t yet had a chance to listen, I hope to be able to report back on this next week.

avoid cvoid
Avoid the C-void! :-D
Yeah, yeah, yeah.
Someone please help me square this circle.
1. Fevers in pregnant women, particularly those in the first trimester, are associated with congenital birth defects and other health issues in babies
2. An extremely common side effect of receiving COVID vaccines is fever.
3. ?????
4. All pregnant women should be vaccinated
Yes, I know that getting COVID would be very bad for pregnant women as well. But at some point we should acknowledge that there is a tradeoff occurring and not blindly march along with the universal jab campaign.
> Fevers in pregnant women, particularly those in the first trimester, are associated with congenital birth defects and other health issues in babies
Do you have any numbers to quantify this risk? For example I’d assume that if this was a measurable effect, it would show up in the flu vaccine safety data, which also causes fever.
CDC has this: https://www.cdc.gov/vaccines/pregnancy/hcp-toolkit/flu-vaccine-pregnancy.html
I think the most likely value for “3. ?????” is “But Covid is orders of magnitude more risky for pregnant women and their unborn children”.
And RE: “blindly marching along”, that’s certainly not my perspective on what’s happening, quite the opposite. As Zvi notes in this post, regulators are restricting access to Moderna in young males due to probably-overstated concerns about myocarditis. Or see the EMA blocking AZ due to one-in-a-million risk of blood clots. These risks are way lower than the risks from Covid, and yet vaccines are being paused/restricted. If there was even the faintest odor of risk to pregnant women I think all the evidence suggests that FDA/EMA etc would freak out and pause vaccines in that group too. My priors are that the regulators are far too conservative here, not the other way around. So a lack of action by these regulators WRT a specific group means that we should expect that there is not even flimsy evidence of risk to that group. (Modulo the FDA not accepting e.g. Israeli data as “valid evidence”, which I view to be a second-order effect here.)
Is fever not a common side effect of covid, I might ask?
Sure, but let’s also account for the fact that not everyone gets COVID and a substantial number of people who get it don’t get a fever. Balance that against the chance that the shot gets a fever.
Also, how high of a fever is experienced when caused by the disease vs. vaccination? I’d be interested to see any peer reviewed studies on this but from the experience of people in my social circle it seems like the fevers were more acute following vaccination. I can almost guarantee that this calculation is completely absent in any of the recommendations, however.
It seems very likely that some causes of fevers in pregnant women will also cause health issues in the babies they give birth to. Is there any reason to think the fever *itself* causes health issues in babies, or is this just something where pregnant people should be avoiding some specific causes of fevers? If it’s the latter, then it would be very helpful to know whether the vaccine is a good or bad cause of fever, and whether covid is a good or bad cause of fever.
If you have time (maybe in next week’s update?), I’d appreciate your best guess as to whether the US is going to see a Northern states winter wave. I can come up with arguments in both directions, so I’ve been personally waffling on what to believe.
You know, I’m actually personally afraid even to think much about this. (My problem, I know. Still, upfront about my bias.)
Nonetheless, here are 2 recent articles (a summary via PBS News Hour by Helen Branswell of STAT News, and a slightly more quantitative NPR article).
The summary seems to be that most models are predicting an overall decline through next March, as Delta is slowly burning out by picking off the unvaccinated who haven’t already had COVID-19. I haven’t dug into the sources behind them yet, just for personal emotional management reasons.
That being said, of course get vaccinated (both COVID-19 and influenza), because you really don’t want to encounter the healthcare system until the load goes down a bit. It’s what I did personally.
Whoops, sorry: the second link to the NPR article was wrong. Here it is.
Wish it were possible to edit posts.
Boy, if there’s one thing I don’t trust it’s predictions about this pandemic that come from SIR-based models done by epidemiologists. These models have had a terrible track record of predicting the course of this pandemic, and other ones too. There are so many arbitrarily-chosen parameters that make a huge difference to outcomes, the model uncertainty is huge.
If you look at the states that had trouble in late summer 2021, they’re the same ones that had trouble in late summer 2020. What that suggests to me is that–probably–the same places that had trouble in winter 2020 will have trouble in winter ’21. I hope it isn’t true, but I’d bet on it at 60% odds.
My best guess is no but I wouldn’t lay large odds against it. Can see it both ways as well.
A “winter wave” is already underway in Northwestern Europe. See the UK or Netherlands numbers. Their fall (and related cold season) has always started much earlier than Northern America’s.
Given that these places have much higher vaccination rates than America, would it be wise to hope for the best, but expect the worst?
My initial thought is to observe the UK as a forecast of what’s going to happen (https://coronavirus.data.gov.uk/details/cases) where instead of a huge India-style spike after the executing operation “covid-shmovid”, they’re just living with an oscillating number of cases around a fairly steady average and seem to be ok with it. I think it’s odd that in the US this pattern doesn’t seem visible, where maybe it’s fair to say that most people are either vaccinated or ‘naturally vaccinated’ though.
I’d be interested to hear any insight you can offer into what we should expect endemic numbers to look like in the long term. I had hoped that the places where people ignored the pandemic and had high numbers for a long time would get over it and be done, compared to places that kept everyone safe but also vulnerable. This seems not to be the case, sadly, but I’m not clear on why. It seemed like everyone should have had it by now, and I haven’t heard of enough reinfections to account for it.
I think we should expect reinfections to be significantly underreported compared to “breakthrough” cases. First, only a fraction of previously infected people know they were previously infected, or can prove it to the medical system, while everyone who was vaccinated knows they were vaccinated. Second, there are various media biases in favor of reporting breakthrough cases – they’re a good man-bites-dog story, they’re a good scare story, and they’re a good anti-vax story, each of which is good motivation for different media venues. I have the sense that these factors aren’t going to be as strong for reporting reinfection cases (although they’re still a good man-bites-dog story, the people who want scare stories are mostly vaccinated and not previously infected; they lack any sort of anti-vax angle).
Various studies have suggested varying levels of protection from prior infection compared to vaccination, which suggests to me that overall, the level of protection is not hugely greater or less. So I would think that, to the extent that delta is able to circulate still in communities with high vaccination, it should also be able to circulate still in communities with high rates of prior infection.
It would be interesting to know how many communities have higher rate of prior infection than of vaccination. As far as I can tell, there are four small counties where more than 1/4 of people have reported a prior infection, and a few dozen others where it’s more than 1/5 – Miami-Dade is the only one of these counties with over 200,000 people. Many of these counties report vaccination rates of 35-40%, and those ones probably have more actual prior infections than vaccinations. But Miami-Dade reports 74% vaccination rate, and the vast majority of counties are both above 40% vaccination and below 20% reported prior infection, so I would guess the vast majority of counties in the United States have more vaccinations than prior infections at this point.
Looks like the link to the ivermectin study fraud in the 3rd to last (“antepenultimate” is a beautiful word, no?) paragraph goes to the wrong place. Right now it goes to the Michael Lin tweet on mix-and-match studies outside the US.
Yep, should be fixed now.
Question, what does the list of symptoms look like for people that didn’t have COVID? IE what was the additional rate of having the symptoms 3% of people had from COVID. if say 0.5% of people have those symptoms normally, then it seems like it would be closer to 1/40 people actually having long COVID and 1/200 people are just background noise
(also thanks for responding to my twitter Q about outdoor transmission, sadly finding airflow studies is really annoying, but all the airflow studies I could find indicate massive effect sizes)
An interesting aspect of the vaccine mandates is being seen with those companies dependent on highly skilled workers that can’t be easily replaced. It seems the way the mandate is written, even contractors of those companies must be vaccinated. With the severe job shortage, a solution being used is to approve any and all exemption requests, no matter how “flimsy”.
Oh yes, that’s a *perfectly* reasonable amount of information it took for you to finally realize long covid, aka covid of the gaps, was probably mostly motivated reasoning all along. Good lord.
In your comment on vaccine rates going from 80->84% you are continuing to assume that COVID transmission basically follows a SEIR model with R0 modulated by behavior and seasonality. This assumption that we are on the verge of exponential decay or growth has not been well validated by actual events.
My belief (and what I think Gottleib and the FDA believe but aren’t saying) is that they expect vaccination to have linear effects rather than exponential effects. Going from 80->84% might reduce cases by 10% but won’t prevent a winter surge which would otherwise occur.
This same reasoning is behind the ambivalence to boosters or approval for children. I don’t think the FDA fundamentally believes that any significant herd immunity benefits from vaccines are possible and therefore assesses solely based on benefits to the individual.
>but would be rather disastrous if red states stopped requiring childhood immunizations.
By the kind of causality espoused by this blog, we should blame the push for vaccination for this, given that it is clearly a marginal effect :)
I remember when the ZOE symptom study had a lower long COVID probability than the ONS study, and everyone claimed the ZOE study had methodological problems. Turns out the ZOE study was right after all.
Cross-posting my comment from LessWrong: what are your thoughts on covid in the USA during the winter, and what the long-term endemic phase will look like?
On the one hand:
– The delta wave is ending, and there are no new variants on the horizon.
– Vaccinations rates are high and slowly rising.
– The overall rate of immunity (from vaccines + natural infection) is high and probably rising (although this is a fight between fading vaccine effectiveness vs natural infections & vaccine booster shots).
On the other hand, winter is traditionally the worst time for colds and flus, including the monster covid wave of 2020. It seems hard to believe we’ll skate through winter 2021 without somewhat of a bump in covid cases.
If you have thoughts about the course of covid beyond this winter (like the prospect for future variants or how necessary it will be for most of the population to take booster shots at a regular cadence), I’d be interested in that too.
One thing that I think will be consequential, in a kind of hilarious way, is that we’re probably going to skip two flu seasons in a row, which will possibly set us up for a whopper flu season down the road. Last winter the flu was practically nonexistent, crowded out by covid. This winter, based on my read of this Metaculus forecast, the flu season is expected to be only half as intense as a typical pre-covid year — peaking at around “4% ILI” instead of around 8%.
https://www.metaculus.com/questions/7621/peak–ili-in-va-during-2021-2022-flu-season/ https://www.vdh.virginia.gov/epidemiology/influenza-flu-in-virginia/influenza-surveillance/
If we get a whopper flu season in 2022 or 2023 (perhaps 2-3x worse than normal), it will be interesting to watch how the media and culture responds — will they go into covid-esque hysterics about the overcrowded hospitals and demand flu lockdowns? Or will it act as a nudge in the other direction, convincing people that the lockdowns and NPIs have got to stop somewhere? Or, perhaps we’ll never get a whopper flu season — maybe Delta will remain the transmissibility king of all the infectious viruses, even after stabilizing and going endemic? Perhaps our transition to remote work, covid-caution in shared indoor spaces, and mRNA vaccines means a permanently more hygienic world?
Overall, I’m very interested in the question of whether covid cases ever crash to suppression levels (as would perhaps have happened in a world without the Delta variant), versus only very slowly trailing off into the background of ordinary pre-covid colds & flus. I think this is very important for predicting how culture will evolve going forwards. A sharper transition from pandemic to negligible covid would encourage more of a snap-back to pre-covid “normality”: more mass concerts, more comfort visiting shared indoor spaces, fewer masks and NPIs, less remote work. Versus a world where covid lingers interminably and there’s no sharp transition into the post-pandemic world will make it harder for culture to coordinate a “return to normal”.
I’m not sure which side I’m cheering for, but it’s clearly an important question regardless. (Remote work and better tech adoption across the board have been highlights of pandemic culture. A slightly increased focus on scientific progress is obviously welcome. And the pre-covid world sometimes strikes me as being a little too heavy on present consumption, like travel vacations, with not enough long-term focus. But of course all the masking and social distancing and reduced socializing has been miserable, and the madness of constantly-changing restrictions is terrible for both business and living an enjoyable human life.)
Something I haven’t seen discussed much, but which seems pretty important if true: One sees occasional reporting in the news that cold-like symptoms are common with delta Covid. I’ve seen a lot of this in what you might call “shitty media outlets,” most credible looking thing I could find was: https://www.bbc.com/news/health-57467051
Is this true? If true, it seems like a big deal and possibly part of the explanation for the higher transmission rates!
The Rogan episode with Gupta (and especially the one with Berenson) was painful. I had to stop listening and I don’t think I’ll listen to Rogan anymore. When I know the details of the studies that Rogan throws around I get really frustrated with his lack of really deep understanding of the science. He is quick and smart, but his lack of depth leads him far astray.
For example, he kept telling Gupta about the Hoeg myocarditis preprint (https://www.medrxiv.org/content/10.1101/2021.08.30.21262866v1) and repeatedly read from a news story about it that boys are more likely to get myocarditis from the vaccine than to get hospitalized by covid. But this misunderstands that the preprint was comparing vaccine risk to covid risk *assuming you had a fairly low chance of getting covid in the first place*. It wasn’t comparing vaccine risk to covid risk conditional on actually getting covid.
Gupta really stumbled and neither made the point that all kids are likely to eventually be exposed to the virus now that it is likely to become endemic, so the net risks from the disease are much higher than the Hoeg preprint estimates, nor did he flesh out that hospitalizations that result from covid are likely to more dangerous than myocarditis, which is often easily treatable.
The Berenson episode was this times a million. Most of the data they showed was “real,” but completely lacking context and depth/understanding to the point of being misinformation. It really reminds me of the numbers games (wrong denominator, failing to compare to other risks, failing to balance risk of an action/policy with risk of the alternatives) Berenson used to fight against when they were coming from covid fearmongers. Now he’s using identical tactics to spread fear about the vaccines.
I wish folks would point out to Rogan that he applies a different standard to vaccines (they must be proven totally safe over decades of testing) than he does to other medications and natural remedies. How can he know that Ivermectin won’t just cause SARS-CoV-2 to go dormant in people’s spinal columns for a decade only to reemerge to kill them? Vaccines hold a special fear in our collective psyche, because we’ve all been exposed to decades of anti-vaxx propaganda. Even those of us very pro-vaxx can’t help falling prey to the emotional fear of jabbing our kids.
Not to disagree with the overall moral of your comment, but on the specifics: Isn’t it true that even when treated, myocarditis essentially always causes scarring that increases the chance of heart disease later in life?
I would never say that these results should be appealed to as an argument against vaccination, period, but perhaps they suggest that we should reserve adenovirus vaccines for young men and boys, or only give them one shot of the RNA vaccines rather than two?
On a related note, here is some *great* news: https://www.reuters.com/world/middle-east/israel-reports-very-few-myocarditis-cases-after-pfizer-boosters-2021-10-01/
Sorry, I didn’t mean to trivialize myocarditis. I just expected that the overall health impacts of getting covid are worse, statistically. But honestly, I’m so concerned about the vaccine risk/benefit for young kids that I’m considering delaying the second dose, depending on what their pediatrician says.
I simply didn’t appreciate Rogan’s incorrect analysis. Gupta couldn’t really keep up with Rogan’s quick questions and didn’t have the deep knowledge of someone like Paul Offit.
I have a bad impression of Offit ethically–I find him to be one of the most authoritarian FDA folks, in that he’s always the one supplying quotes about how people shouldn’t be permitted to take medicine until every bureaucratic ‘i’ has been dotted and every ‘t’ crossed–but he’s always seemed well-informed, certainly. Unwilling to engage in Bayesian reasoning while on the job, but well-informed.
I understand that you think FDA folks like Offit are too conservative when it comes to vaccine or treatment safety to the point of delaying effective medicines. But that would make him the perfect person for Rogan or others worried about the vaccines to talk to. :)
Great analysis on the overall unhelpfulness of the Gupta/Rogan discussion:
https://podcasts.apple.com/us/podcast/the-zdoggmd-show/id1218431966?i=1000538646479
I used to enjoy Rogan, but it’s been increasingly frustrating listening to him spread covid misinformation, host vaccine skeptics, and promote ivermectin.
I have a few vaccine hesistant friends. The take away they seem to get from the show is that Joe can get doctors to say “I don’t know” a lot, and that implies that they’re really just unsure about the safety of the vaccine, and thus it makes sense to not take it.
This was especially funny after Rhonda Patrick went on. Joe asked Rhonda why he hadn’t gotten covid yet, despite lots of exposure. Joe insisted he must be immune. Rhonda couldn’t explain it. One week later, Joe got covid.
I’m pretty sure Joe later admitted he’d been taking ivermectin to prevent covid (I think that was in the Tom Segura episode). I still have trouble seeing Joe as a right wing agitator, or someone intentionally pushing a bad agenda. If anything, I see him as an everyman, confused by the information landscape, as much a victim of misinformation as the source.
And I think there’s also some unhelpful interplay between censorship and misinformation here. Google and Twitter try to take down bad actors and people like Joe see that as a sign of conspiracy and boost their signals. I tried writing a bit about that:
View at Medium.com
Rogan is a comedian. Gupta is a doctor. And your takeaway is that Rogan’s Covid interpretations are incorrect and that Rogan should not be listened to in general? Clever insight. I don’t dispute it. Of course, the Covid interpretations of Gupta & Co have often been wrong as well. And Gupta & Co are qualified to be cited as authorities by, say, Wikipedia. There seems to be a tribal twist in your take.
Rogan used to be a comedian. Now he is a talkshow host.
I didn’t mean to imply the Gupta has been right about covid. I haven’t watched him so I don’t have an opinion. But I don’t think Wikipedia typically puts a lot of weight on what one CNN correspondent says.
So yesterday the FDA’s VRBPAC advised the FDA to approve Moderna boosters, at half the dose of the first 2 shots. If you want a summary of what went down, I wrote a summary.
Some highlights:
(1) The Israeli data first seen at the Pfizer booster hearings has matured nicely. They’ve shown what looks like convincing evidence of efficacy waning, even against severe disease and hospitalization. They’ve also shown that stopped after rolling out boosters (though it may just have been Delta peaking).
(2) The Israeli data on side effects were, if anything, comparable to or milder than the first 2 shots.
(3) The Israeli myocarditis/pericarditis among males 18-24 was at a probability of about 3 per 100,000. That’s higher than other groups but still pretty low, and NOT higher than previous doses. So boosters don’t make it worse.
(4) US myocarditis/pericarditis among males 18-24 was measured differently, because reasons, but it came out to about 5 events per million person-days (95% confidence limits: 1 – 10). For all other groups/genders, it was about 2 events per million person-days (95% cl: 0 – 5). Pfizer vs Moderna showed no difference.
(5) Moderna was 98.2% efficacy vs hospitalization, at least until Delta showed up to spoil things. But a booster raised antibodies to Delta, too. Apparently having Delta in circulation at the time of a dose helps, for some reason I don’t understand?
(6) The approval was unanimous at 19-0.
And today the FDA’s VRBPAC advised the FDA to approve J&J boosters, and discussed the data on mix-and-match boosters where the primer and the booster are different vaccines. If you want to look through the tea leaves, I wrote a summary.
Some highlights:
(1) J&J seems to show lower efficacy than the mRNA vaccines, but also less waning. So the point of a booster would be to bump up the efficacy, not to stop waning.
(2) Things only went partially in J&J’s favor: boosters approved unanimously 19-0, but sentiment is moving in the direction of forcing it to be a 2-shot vaccine and to encourage boosters with an mRNA vaccine, not necessarily the J&J vaccine again. So they’ve approved a booster, but looked at data on other things that might prove to be even better, once they have data to decide.
(3) The mix-and-match trail from NIH/NIAID looked really good! The heterologous boosters were as good or even better than the homologous ones, with no particularly scare adverse events. Unfortunately, this is an early-stage result, which will require more data for the FDA to approved mixed primer/booster series.
A bit mixed for J&J, but probably a good result for the general welfare.
Today the FDA formally authorized Moderna boosters, J&J boosters, and all the mix-and-match combination boosters. This is very aggressive for them!
The next step is for the CDC’s ACIP to meet and issue a recommendation for practices, and for the CDC directory to accept that recommendation. At that point it’ll be (almost) boosters all around. The ACIP meets tomorrow, 2021-Oct-12.
Regarding the last ‘ominous question’ you recorded on your nice article, I’m surprised the third alternative wasn’t considered – “Should we have spaced out the doses longer than 3 weeks?”. It’s not impossible that two shots 3 weeks apart (vs 3 months like the UK) does fairly little in the long run, and if so, 9+ months between single shots may do even less. This would be excellent news for the vaccine manufacturers.
[A very minor clarification: “chilling postscript” was Helen Branswell’s description, not mine. Though I do agree with her, so I’ll own the fact that I quoted her approvingly.]
Re dose spacing:
Without question, you are correct: the initial 2 doses of both mRNA vaccines should probably have been further spaced out to get more immune response. Just as a bitter little lagniappe, if we had gone to a first-doses-first strategy, we’d have spaced the doses out more and gotten more people to partial immunity faster.
There are only 2 things, really, to say about it:
(1) The decision to go with 3 weeks for Pfizer and 4 weeks for Moderna was probably the minimum separation, rather than the optimal. Finding the optimum would have taken a longer time in the trials, probably. The shorter time to get people fully vaccinated might have saved some lives, as opposed to optimizing the immunity of a smaller number of people. At least, that’s my guess, knowing how those decisions get argued over. (And yes, that is ironically the opposite of first-doses-first. Which one’s right depends on the value of partial vs full immunity, which I think nobody could have known.)
(2) The VRBPAC is not going to review the spacing of the first 2 doses, since it’s already in place for hundreds of millions of people. They have to deal with the medical reality that so many people already have doses spaced as they were. So they start with the status quo as a prior, and ask what we can do to improve things from here.
Re “excellent news for the vaccine companies”:
I realize this was just a little rhetorical flourish, and that’s perfectly fine.
But I’m pretty sure they’re not making huge profits here. Meeting their costs, absolutely. Making some profit, very probably.
Let me tell you about the time I was in on one of the Moderna quarterly earnings calls in late 2020. I remember the argument about what to charge for the now charmingly-named Spikevax. They went through an elaborate exercise called an ICER analysis (“incremental cost effectiveness ratio”) to convince investors that it was very, very valuable. (Hey, it was an earnings call. That’s what those are for.)
Then, volte face, they admitted they wouldn’t be able to charge that much during a pandemic without the risk of essentially getting nationalized (they didn’t use that phrase, I interpolated it). So they had a responsibility to manufacture “at risk” (ahead of approval), and charge some very, very modest price like $35/dose so middle class people could afford it and the government could subsidize it for the poor.
Honestly, most of the cost of the vaccination campaign is probably in logistics (transportation to every pharmacy in the country, a rigorous cold chain with verification steps to catch spoilage, etc.) and personnel costs (people who know how to give the jab, people who know how to handle fainting and all the other stuff that can go wrong, people to manage the crowd and do security, etc.). I can’t prove it, but I bet the actual cost of the vaccine is not the biggest cost.
@WeekendEditor yeah I regretted the snarky remark as soon as I posted, but alas there is no edit function. You did an excellent job of making lemonade with it.
I watched the entire 3+ hour Rogan/Gupta podcast, and found it fascinating on many levels.
Zvii, I really hope you find time to watch it, and have extensive commentary next week.
Also…
I’m writing from Nova Scotia, in Atlantic Canada, where we have perhaps the best Covid numbers in all of North America (about 10 fatalities / 100,000).
Probably more by accident than design, provincial governments have followed most of the policies you have recommended alll along…ignoring AZ clotting panic, first doses first, mixed vaccines…and it has worked out very well for us.
It’s great to have someone out there who is providing good, prescient advice, while also calling the experts to account when they screw up.
Thanks!
Zvi, what do you use as a data source for your graphs, these days? I remember you used to use the Covid Tracking Project, but I can’t remember what you switched to when they shut down.
(context: I often cite your stats to my girlfriend when discussing covid, and she asked where you get them. I couldn’t remember and said I would ask.)
Wikipedia. https://en.wikipedia.org/wiki/Template:COVID-19_pandemic_data/United_States_medical_cases and https://en.wikipedia.org/wiki/Template:COVID-19_pandemic_data/United_States_daily_deaths
“One big cost of all this is that Republicans are turning against vaccinations and vaccine mandates in general, ”
I followed your link, and I saw support of the latter claim, (turning against vaccine mandates) but none for the former claim. (Turning against vaccinations.) It appears to me that the libertarian stance is being conflated with being anti-science, and perhaps deliberately on Hanania’s part. (Because surely he read the WaPo article he linked to.)
Yeah, for established vaccinations I’ve been doing that too, and equating mandate opposition with vaccine opposition. I try to be careful to draw the distinction with the Covid vaccine in particular and didn’t think about it for e.g. Mumps vaccines. It’s certainly possible to have the libertarian position, but I think that is few if anyone’s true objection here. Also I think it’s not an especially reasonable position for the well-established vaccines, and if you were holding such positions then you’re pretty outside the basic philosophy of the party and should have voted for Jorgenson.
Actually, I think the libertarian objection is gaining ground. Mostly on account of the administration refusing to credit natural immunity; This tends to convince people who might be open to a medical case for a mandate that the actual mandate isn’t medically motivated.
And there are so many things that they should be doing before mandating vaccinations that they’re not doing, that it really is hard to believe policy is being guided by medical reasoning.
I do think it’s a problem that, having concluded that the Covid vaccine mandate isn’t medically justified, (The mandate, not the vaccine!) this leaks over into vaccinations that genuinely do have a medical case for mandates, and were adopted before the FDA/CDC became totally political. But they have become totally political, and that’s a consequence of it: People won’t listen even when they should.
As for Jorgenson, I gave up on the LP after the second Harry Browne run, when I concluded that the system had been too rigged for 3rd parties to be anything but a waste of time, and that the LP in particular had been taken over by grifters and loons. Three non-libertarian nominees in a row cemented that decision.
The LP only exists at this point to bleed off political activism that might otherwise be effective, and serve as a spoiler in key races. (A role they actually bragged about in 2016.) Their picking a nominee who’s actually a libertarian doesn’t change that; A principled time suck is still a time suck.
Hi Zvi,
You may be correct about how the libertarian objection represents an insignificant one within you’re readership as a whole, but I thought I would register my own case as a counterexample. I am a dues paying LP member who is happy that people have the chance to vaccinate if they want it, but completely appalled by the mandates, to the point that I am about to resign from my job at Ginormico over these. To me it’s the worst federal policy decision that’s been made since the US decided to invade Iraq, and I will find a way to spend my time from 8 – 6 with an employer that’s not so excited about being the state’s goon squad, even at the risk of several paychecks and the chance that my next job doesn’t pay as well as my current one. So be it. It may be easy to dismiss as being based on silly principles, but to me it’s more rational and utilitarian. Apparently we place a much larger negative value on attaining a state of totalitarian technocracy in the US than you, and also a much higher incremental probability of its occurrence, conditional on sweeping (and frankly arbitrary) vaccine mandates becoming part of the culture and legal precedent. This is why mandating MMR and chicken pox shots in public schools only bothered me a little; they existed for decades without taking us appreciably closer to Brave New World.
JoJo was a clown show. I voted for Giant Meteor out of protest to not reward the LP for completely missing the opportunity to be relevant in 2020.
I do appreciate your perspective, even if (or perhaps because?) it’s not my own. Thanks for all the work you put into this blog.
Anders, I am curious, do you extend that logic to the non-Covid older vaccines and their mandates? I do think the true Libertarian objection is rare even on Covid vaccines (although real and legit there) but I expect it to be even rarer on the older vaccines (and I see it as much less legit there).
I was bothered a little but not a lot by the older vaccine mandates. But you are correct, it wasn’t a hill I was about to die on because there were multiple good ways around it in practice, e.g. homeschooling, for people who were really chafed by getting their kids vaccinated (FWIW my kids are all up to date). And those tended also to be channels that kept the mumps outbreaks more isolated. I don’t have all that many libertarian friends, but the ones I have talked about it with feel similarly, although at least one is of the more deontological “Justice be done though the heavens may fall” bent.
The other thing about the pre-COVID mandates is that they coalesced at a time when people thought the first amendment still applied, so it did not *require* trust in the federal bureaucracy to see the case for universal vaccination. The marginalization of dissent was not total at that point and the expert class had not totally merged into a blob to create an effective sample size of one. Nowadays, anything that disagrees with the alphabet soup consensus on the actual effects of vaccines is labeled as misinformation and immediately removed from the commons, so in the case of the COVID shots I think there is massive overconfidence, even if the conclusion ends up being directionally correct. The principle of bodily autonomy is only partly what we see as being at stake now, whereas that was basically 100% of it when we were just talking about chicken pox. With the mRNA vaccines it isn’t even so much about freedom of speech per se, but about the reason we had (not have) freedom of speech.
Hang on, that was never the “Long Covid” I’m worried about! Does anyone care very much how long symptoms last? Permanent or decades-long damage to the brain, heart, and lungs is much more worrying. Any data on that? I’m aware of the IQ paper but nothing else.
How could there be data on decades? Covid’s only been observed for about 18 months. No one can say with confidence *anything* about effects longer than that.
At least you know that if the symptoms clear up in 12 or 19 weeks that they’re probably not coming back later, so that’s an upper bound on how bad it could be.